I have written about disaster early warnings on many occasions during the past decade (see 2014 example). I have likened it to running a relay race. In a relay, several runners have to carry the baton and the last runner needs to complete the course. Likewise, in disaster early warnings, several entities – ranging from scientific to administrative ones – need to be involved and the message needs to be identified, clarified and disseminated fast.
Good communications form the life blood of this kind of ‘relay’. Warnings require rapid evaluation of disaster situation, quick decision making upon assessing the risks involved, followed by rapid dissemination of the decision made. Disaster warning is both a science and an art: those involved have to work with imperfect information, many variables and yet use their best judgement. Mistakes can and do happen at times, leading to occasional false alarms.
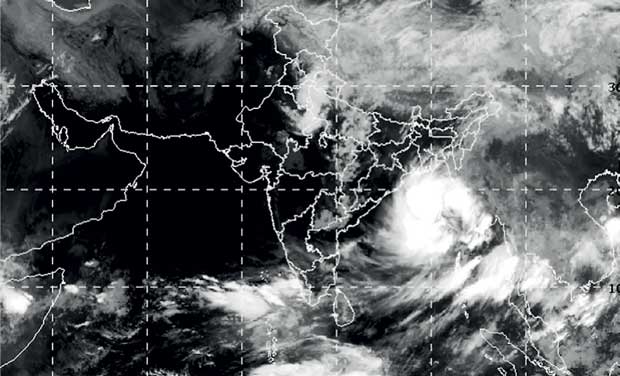
In the aftermath of the heavy monsoonal rains in late May 2017, southern Sri Lanka experienced the worst floods in 14 years. The floods and landslides affected 15 districts (out of 25), killed at least 208 and left a further 78 people missing. As of 3 June 2017, some 698,289 people were affected, 2,093 houses completely destroyed, and 11,056 houses were partially damaged.
Did the Department of Meteorology and Disaster Management Centre (DMC) fail to give adequate warnings of the impending hydro-meteorological hazard? There has been much public discussion about this. Lankadeepa daily newspaper asked me for a comment, which they published in their issue of 7 June 2017.
I was asked to focus on the use of ICTs in delivering disaster early warnings.
We as a nation collectively uttered these words as we raised our heads after the Indian Ocean tsunami of December 2004. That mega-disaster, which caught our government unawares and society unprepared, devastated many coastal areas, killing around 40,000 and displacing over a million people.
Even a 30 minute early warning could have saved many of those lost lives, by simply asking them to run inland, away from the waves. But there was no such warning.
Badly shaken by that experience, the then government reformed disaster related laws and institutions. Until then, dealing with disaster response was lumped under social services. The new system created a dedicated ministry for disaster management, with emphasis on disaster risk reduction (DRR).
Living amidst multiple hazards is unavoidable, but preparedness can vastly reduce impacts when disasters do occur. That is DRR in a nutshell.
But in immature democracies like ours, we must never say never again. Our political parties and politicians lack the will and commitment required to meet these long-term objectives. Our governance systems are not fully capable of keeping ourselves safe from Nature’s wrath.
Disaster resilience is not a technocratic quick fix but the composite outcome of a myriad actions. Good governance is the vital ‘lubricant’ that makes everything come together and work well. Without governance, we risk slipping back into business as usual, continuing our apathy, greed and short-termism.
This big picture level reality could well be why disaster response has been patchy and uncoordinated in both May 2016 and last week.
Fundamental issues
As the flood waters recede in affected parts of Sri Lanka, familiar questions are being asked again. Did the government’s disaster management machinery fail to warn the communities at risk? Or were the hazard warnings issued but poorly communicated? And once disaster occurred, could the relief response have been better handled? Are we making enough use of technological tools?
Finger pointing won’t get us very far, even though public anger is justified where governmental lapses are evident. We need to move beyond the blame game to identify core issues and then address them.
In my view, two high level issues are climate resilience and improved governance.
DRR is easier said than done in the best of times, and in recent years human-made climate change has made it much harder. Global warming is disrupting familiar weather patterns and causing more frequent and intense weather. What used to be weather extremes occurring once in 25 or 50 years in the past now happens every few years.
Climate imperatives
The UN’s climate panel (IPCC) says that global average temperatures could rise by somewhere between 2 degree and 6 degrees Centigrade by 2100. This would trigger many disruptions, including erratic monsoons, the seasonal oceanic winds that deliver most of our annual rains.
That is more than two thirds of the total number of 646,500 people affected by floods and landslides in the South, as counted on June 1. But slowly-unfolding droughts never get the kind of press that floods inspire.
One thing is clear: disaster management can succeed today only if climate realities are factored in. And coping with climate change’s now inevitable impacts, a process known as climate adaptation, requires technical knowledge combined with proper governance of both natural resources and human systems.
Sri Lanka: Not only oscillating between droughts and floods, but now also having both disasters at the same time. Cartoon by Gihan de Chickera
Adapt or Perish
Sri Lanka joined the UN Framework Convention on Climate Change (UNFCCC) in 1992. But 25 years on, climate considerations are not fully factored into our development planning and public investments. State agencies in charge of roads, railways, irrigation works and utilities don’t appear to realise the need to ‘insure’ their installations and operations from climate impacts.
Climate adaptation is not something that the disaster ministry and DMC alone can accomplish. It needs to be a common factor that runs across the entire government, from agriculture and health to power and transport. It needs to be the bedrock of DRR.
We need aware and empowered local communities matched by efficient local government bodies. This combination has worked well, for example, in the Philippines, now hailed as a global leader in DRR.
Image courtesy – Health Education Bureau of Sri Lanka
In this week’s Ravaya column (in Sinhala, published in issue dated 15 May 2016),, I revisit a public health emergency that I have been writing about for several years: mass kidney failure for no known reason.
Beginning in the 1990s, thousands of people in Sri Lanka’s Dry Zone – heartland of its rice farming — developed kidney failure without having diabetes or high blood pressure, the common causative factors. Most affected were men aged 30 to 60 years, who worked as farmers. As numbers rose, puzzled doctors and other scientists started probing possible causes for what is now named Chronic Kidney Disease of unknown etiology (abbreviated as CKDu).
CKDu has become a fully fledged humanitarian emergency, affecting thousands of people and their families – most of them subsistence farmers.
Investigating causes of this ailment — still not pinned down to a specific cause or factor — has proven difficult. While scientists follow rigorous scientific methods, some ultra-nationalists and opportunistic politicians are trying to hijack the issue for their own agenda setting. Some journalists have added fuel to the fire with sensationalist reporting and unwarranted fear-mongering.
On 9 May 2016, I moderated High Level Media Dialogue on Chronic Kidney Disease of Unknown Aetiology (CKDu) and Public Health in Colombo. It was organised jointly by the Ministry of Health, Nutrition and Indigenous Medicine; Ministry of Parliamentary Reforms and Mass Media; and theCoordinating Secretariat for Science, Technology and Innovation (COSTI) of the Ministry of Science, Technology and Research.
Three experienced medical professionals joined our conversation: Dr Tilak Abeysekera, Consultant Nephrologist, Nephrology Dialysis and Transplant Unit, General Hospital, Kandy; Dr Palitha Mahipala, Director General, Health Services, Ministry of Health, Nutrition and Indigenous Medicine; and Dr Vinya Ariyaratne, General Secretary of Sarvodaya and consultant community physician.
In this column, I summarise some of the latest scientific analysis and humanitarian issues that were presented during the event.
See also my other writing on the subject (some early ones are updated in this latest Ravaya column):
Managing disaster early warnings is both a science and an art. When done well, it literally saves lives — but only if the word quickly reaches all those at risk, and they know how to react.
We have come a long way since the devastating Boxing Day tsunami of December 2004 caught Indian Ocean countries by surprise. Many of the over 230,000 people killed that day could have been saved by timely coastal evacuations.
Early warnings work best when adequate technological capability is combined with streamlined decision-making, multiple dissemination systems and well prepared communities.
Rapid onset disasters — such as tsunamis and flash floods — allow only a tight window from detection to impact, typically 15 to 90 minutes. When it comes to tsunamis, it is a real race against time. Effective tsunami warnings require very rapid evaluation of undersea earthquakes and resulting sea level changes, followed by equally rapid dissemination of that assessment.
Following the 2004 disaster, the Indian Ocean Tsunami Warning and Mitigation System (IOTWS) was set up in 2005 under UNESCO’s Intergovernmental Oceanographic Commission. It is a regional collaboration that brings together three regional tsunami service providers – scientific facilities operated by the governments of Australia, India and Indonesia — and over a dozen national tsunami centres. The latter are state agencies designated by governments to handle in-country warnings and other mitigation activities.
Participants of SHER (Science, Health, Environment & Risk) Communication – Role of S&T Communication in Disaster Management and Community Preparedness held in Jakarta, Indonesia, on 8-9 Dec 2015
It was organised by the Association of Academies and Societies of Sciences in Asia (AASSA) in collaboration with the Indonesian Academy of Sciences (AIPI), Korean Academy of Science and Technology (KAST) and the Agency for Assessment and Application of Technology (BPPT) in Indonesia.
The workshop brought together around 25 participants, most of them scientists researching or engaged in publication communication of science, technology and health related topics. I was one of two journalists in that gathering, having been nominated by the National Academy of Sciences of Sri Lanka (NAASL).
I drew on over 25 years of journalistic and science communication experience, during which time I have worked with disaster managers and researchers, and also co-edited a book, Communicating Disasters: An Asian Regional Handbook (2007).
Nalaka Gunawardene speaking at Science, Health, Environment & Risk Communication Asian regional workshop held in Jakarta, Indonesia, 8-9 Dec 2015
The challenge in disaster early warnings is to make the best possible decisions quickly using imperfect information. With lives and livelihoods at stake, there is much pressure to get it right. But one can’t be timely and perfectly accurate at the same time.
We have come a long way since the devastating Boxing Day tsunami of December 2004 caught Indian Ocean countries by surprise. Many of the over 230,000 people killed that day could have been saved by timely coastal evacuations.
The good news is that advances in science and communications technology, greater international cooperation, and revamped national systems have vastly improved tsunami early warnings during the past decade. However, some critical gaps and challenges remain.
The Indian Ocean Tsunami Warning and Mitigation System (IOTWS) was set up in 2005 under UNESCO’s Intergovernmental Oceanographic Commission. Over USD 400 million has been invested in state of the art equipment for rapid detection and assessment. However, the system’s overall effectiveness is limited by poor local infrastructure and lack of preparedness. Some countries also lack efficient decision-making for issuing national level warnings based on regionally provided rapid assessments.
Warnings must reach communities at risk early enough for action. False warnings can cause major economic losses and reduce compliance with future evacuation orders. Only governments can balance these factors. It is important that there be clearer protocols within governments to consider the best available information and make the necessary decisions quickly.
Now, the proliferation of information and communication technologies (ICTs) is making this delicate balance even more difficult. To remain effective in the always-connected and chattering Global Village, disaster managers have to rethink their engagement strategies.
Controlled release of information is no longer an option for governments. In the age of 24/7 news channels and social media, many people will learn of breaking disasters independently of official sources. Some social media users will also express their views instantly – and not always accurately.
How can this multiplicity of information sources and peddlers be harnessed in the best public interest? What are the policy options for governments, and responsibilities for technical experts? How to nurture public trust, the ‘lubricant’ that helps move the wheels of law and order – as well as public safety – in the right direction?
As a case study, I looked at what happened on 11 April 2012, when an 8.6-magnitude quake occurred beneath the ocean floor southwest of Banda Aceh, Indonesia. Several Asian countries issued quick warnings and some also ordered coastal evacuations. For example, Thai authorities shut down the Phuket International Airport, while Chennai port in southern India was closed for a few hours. In Sri Lanka, panic and chaos ensued.
In the end, the quake did not generate a tsunami (not all such quakes do) – but it highlighted weaknesses in the covering the ‘last mile’ in disseminating early warnings clearly and efficiently.
Speakers on ‘ICT Applications for Disaster Prevention and Treatment’ in Jakarta, Indonesia, 8-9 Dec 2015
I concluded: Unless governments communicate in a timely and authoritative manner during crises, that vacuum will be filled by multiple voices. Some of these may be speculative, or mischievously false, causing confusion and panic.
In this week’s Ravaya column (in Sinhala), published on 23 November 2014, I ask whether astrologers are the most powerful persons in Sri Lanka. This is because all important decisions of the state, including the ceremonial opening of Parliament and scheduling of elections, is done strictly on astrological advice.
Speaking at a recent meeting of the Sri Lanka Rationalists’ Association to discuss my latest book, writer and political commentator Gamini Viyangoda said astrology determines so many personal and public decisions in Sri Lanka. In this obsession, ruling party and opposition party politicians seem united.
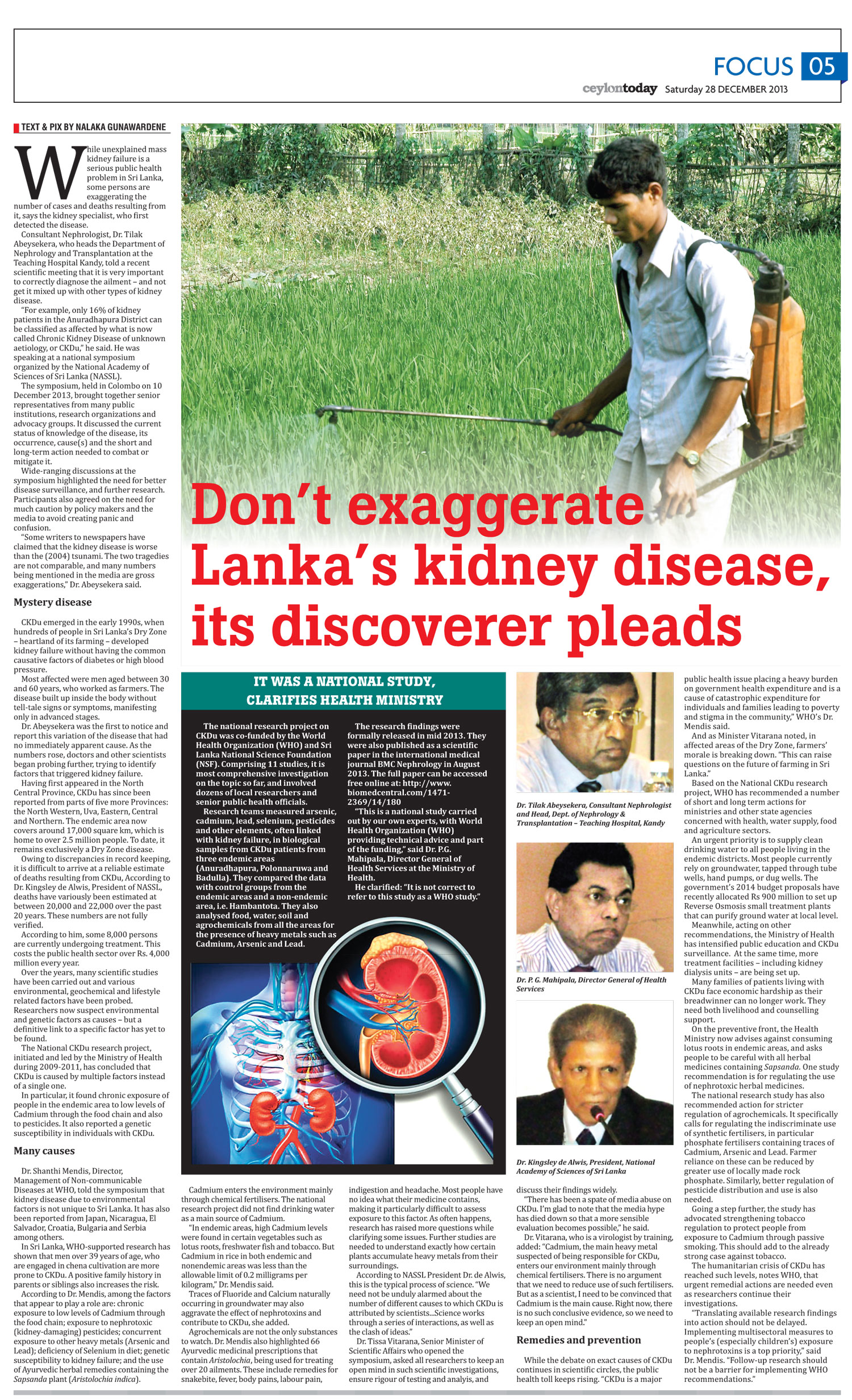
While unexplained mass kidney failure is a serious public health problem in Sri Lanka, some persons are exaggerating the number of cases and deaths resulting from it, says the kidney specialist who first detected the disease.
Consultant Nephrologist Dr Tilak Abeysekera, who heads the Department of Nephrology and Transplantation at the Teaching Hospital Kandy, told a recent scientific meeting that it is very important to correctly diagnose the ailment – and not get it mixed up with other types of kidney disease.
“For example, only 16% of kidney patients in the Anuradhapura district can be classified as affected by what is now called Chronic Kidney Disease of unknown aetiology, or CKDu,” he said. He was speaking at a national symposium organised by the National Academy of Sciences of Sri Lanka (NASSL).
The symposium, held in Colombo on 10 December 2013, brought together senior representatives from many public institutions, research organisations and advocacy groups. It discussed the current status of knowledge of the disease, its occurrence, cause(s) and the short and long-term action needed to combat or mitigate it.
Wide-ranging discussions at the symposium highlighted the need for better disease surveillance, and further research. Participants also agreed on the need for much caution by policy makers and the media to avoid creating panic and confusion.
“Some writers to newspapers have claimed that the kidney disease is worse than the (2004) tsunami. The two tragedies are not comparable, and many numbers being mentioned in the media are gross exaggerations,” Dr Abeysekera said.
Mystery disease
CKDu emerged in the early 1990s, when hundreds of people in Sri Lanka’s Dry Zone – heartland of its farming — developed kidney failure without having the common causative factors of diabetes or high blood pressure.
Most affected were men aged between 30 and 60 years who worked as farmers. The disease built up inside the body without tell-tale signs or symptoms, manifesting only in advanced stages.
Dr Abeysekera was the first to notice and report this variation of the disease that had no immediately apparent cause. As the numbers rose, doctors and other scientists began probing further, trying to identify factors that triggered kidney failure.
Having first appeared in the North Central Province, CKDu has since been reported from parts of five more provinces: the North Western, Uva, Eastern, Central and Northern. The endemic area now covers around 17,000 square km, which is home to over 2.5 million people. To date, it remains exclusively a Dry Zone disease.
Owing to discrepancies in record keeping, it is difficult to arrive at a reliable estimate of deaths resulting from CKDu, According to Dr. Kingsley de Alwis, President of NASSL, deaths have variously been estimated at between 20,000 and 22,000 over the past 20 years. These numbers are not fully verified.
According to him, some 8,000 persons are currently undergoing treatment. This costs the public health sector over Rs. 4,000 million every year.
Over the years, many scientific studies have been carried out and various environmental, geochemical and lifestyle related factors have been probed. Researchers now suspect environmental and genetic factors as causes – but a definitive link to a specific factor has yet to be found.
The National CKDu research project, initiated and led by the Ministry of Health during 2009-2011, has concluded that CKDu is caused by multiple factors instead of a single one (see also box below).
In particular, it found chronic exposure of people in the endemic area to low levels of Cadmium through the food chain and also to pesticides. It also reported a genetic susceptibility in individuals with CKDu.
Many causes
Dr Shanthi Mendis, Director, Management of Non-communicable Diseases at WHO, told the symposium that kidney disease due to environmental factors is not unique to Sri Lanka. It has also been reported from Japan, Nicaragua, El Salvador, Croatia, Bulgaria and Serbia among others.
In Sri Lanka, WHO-supported research has shown that men over 39 years of age who are engaged in chena cultivation are more prone to CKDu. A positive family history in parents or siblings also increases the risk.
According to Dr Mendis, among the factors that appear to play a role are: chronic exposure to low levels of Cadmium through the food chain; exposure to nephrotoxic (kidney-damaging) pesticides; concurrent exposure to other heavy metals (Arsenic and Lead); deficiency of Selenium in diet; genetic susceptibility to kidney failure; and the use of Ayurvedic herbal remedies containing the Sapsanda plant (Aristolochia indica).
Cadmium enters the environment mainly through chemical fertilisers. The national research project did not find drinking water as a main source of Cadmium.
“In endemic areas, high Cadmium levels were found in certain vegetables such as lotus roots, freshwater fish and tobacco. But Cadmium in rice in both endemic and nonendemic areas was less than the allowable limit of 0.2 milligrams per kilogram,” Dr Mendis said.
Traces of Fluoride and Calcium naturally occurring in groundwater may also aggravate the effect of nephrotoxins and contribute to CKDu, she added.
Agrochemicals are not the only substances to watch. Dr Mendis also highlighted 66 Ayurvedic medicinal prescriptions that contain Aristolochia, being used for treating over 20 ailments. These include remedies for snakebite, fever, body pains, labour pain, indigestion and headache. Most people have no idea what their medicine contains, making it particularly difficult to assess exposure to this factor.
As often happens, research has raised more questions while clarifying some issues. Further studies are needed to understand exactly how certain plants accumulate heavy metals from their surroundings.
According to NASSL President Dr de Alwis, this is the typical process of science. “We need not be unduly alarmed about the number of different causes to which CKDu is attributed by scientists…Science works through a series of interactions, as well as the clash of ideas.”
Dr Tissa Vitarana, Senior Minister of Scientific Affairs who opened the symposium, asked all researchers to keep an open mind in such scientific investigations, ensure rigour of testing and analyis, and discuss their findings widely.
“There has been a spate of media abuse on CKDu. I’m glad to note that the media hype has died down so that a more sensible evaluation becomes possible,” he said.
Dr Vitarana, who is a virologist by training, added: “Cadmium, the main heavy metal suspected of being responsible for CKDu, enters our environment mainly through chemical fertilisers. There is no argument that we need to reduce use of such fertilisers. But as a scientist, I need to be convinced that Cadmium is the main cause. Right now, there is no such conclusive evidence, so we need to keep an open mind.”
Remedies & prevention
While the debate on exact causes of CKDu continues in scientific circles, the public health toll keeps rising.
“CKDu is a major public health issue placing a heavy burden on Government health expenditure and is a cause of catastrophic expenditure for individuals and families leading to poverty and stigma in the community,” WHO’s Dr Mendis said.
And as Minister Vitarana noted, in affected areas of the Dry Zone, farmers’ morale is breaking down. “This can raise questions on the future of farming in Sri Lanka.”
Based on the National CKDu research project, WHO has recommended a number of short and long term actions for ministries and other state agencies concerned with health, water supply, food and agriculture sectors.
An urgent priority is to supply clean drinking water to all people living in the endemic districts. Most people currently rely on groundwater, tapped through tube wells, hand pumps, or dug wells. The government’s 2014 budget proposals have recently allocated Rs 900 million to set up Reverse Osmosis small treatment plants that can purify ground water at local level.
Meanwhile, acting on other recommendations, the Ministry of Health has intensified public education and CKDu surveillance. At the same time, more treatment facilities – including kidney dialysis units – are being set up.
Many families of patients living with CKDu face economic hardship as their breadwinner can no longer work. They need both livelihood and counselling support.
On the preventive front, the Health Ministry now advises against consuming lotus roots in endemic areas, and asks people to be careful with all herbal medicines containing Sapsanda. One study recommendation is for regulating the use of nephrotoxic herbal medicines.
The national research study has also recommended action for stricter regulation of agrochemicals. It specifically calls for regulating the indiscriminate use of synthetic fertilisers, in particular phosphate fertilisers containing traces of Cadmium, Arsenic and Lead. Farmer reliance on these can be reduced by greater use of locally made rock phosphate. Similarly, better regulation of pesticide distribution and use is also needed.
Going a step further, the study has advocated strengthening tobacco regulation to protect people from exposure to Cadmium through passive smoking. This should add to the already strong case against tobacco.
The humanitarian crisis of CKDu has reached such levels, notes WHO, that urgent remedial actions are needed even as researchers continue their investigations.
“Translating available research findings into action should not be delayed. Implementing multisectoral measures to people’s (especially children’s) exposure to nephrotoxins is a top priority,” said Dr Mendis. “Follow-up research should not be a barrier for implementing WHO recommendations.”
Text box:
It was a national study, clarifies Health Ministry
The national research project on CKDu was co-funded by the World Health Organization (WHO) and Sri Lanka National Science Foundation (NSF). Comprising 11 studies, it is most comprehensive investigation on the topic so far, and involved dozens of local researchers and senior public health officials.
Research teams measured arsenic, cadmium, lead, selenium, pesticides and other elements, often linked with kidney failure, in biological samples from CKDu patients from three endemic areas (Anuradhapura, Polonnaruwa and Badulla). They compared the data with control groups from the endemic areas and a non-endemic area, i.e. Hambantota. They also analysed food, water, soil and agrochemicals from all the areas for the presence of heavy metals such as Cadmium, Arsenic and Lead.
The research findings were formally released in mid 2013. They were also published as a scientific paper in the international medical journal BMC Nephrologyin August 2013. The full paper can be accessed free online at: http://www.biomedcentral.com/1471-2369/14/180
“This is a national study carried out by our own experts, with World Health Organization (WHO) providing technical advice and part of the funding,” said Dr P.G. Mahipala, Director General of Health Services at the Ministry of Health.
He clarified: “It is not correct to refer to this study as a WHO study.”
Don’t exaggerate Lanka’s kidney disease – by Nalaka Gunawardene – Ceylon Today, 28 Dec 2013
Arriving in the Philippines just two weeks after the super typhoon Haiyan (local name Yolanda) hit the archipelago nation on 8 November 2013, I’ve been following many unfolding debates on disaster recovery and resilience.
The Filipino media have been full of post-disaster stories. Among them, I came across an editorial in the Philippine Star on 26 Nov 2013, titled Stopping the Waves, which touched on the role of protecting natural barriers that can guard coastal areas from storm surges.
A key excerpt: “Nothing can stop a storm surge, but there are ways of minimizing the impact of powerful waves. Levees have been built in some countries, although the ones in New Orleans were breached by the storm surge during Hurricane Katrina. Another option is to develop mangrove forests, which can also function as bird sanctuaries and breeding grounds for marine life.”
It added: “Yolanda has revived the debate over the proposed destruction of the coastal lagoon to make way for commercial development. That mangrove forest must be protected and expanded rather than destroyed, and more mangrove areas must be propagated throughout the archipelago. You can’t roll back deadly waves, but their punch can be blunted. Natural barriers should help do the job.”
This is just what TVE Asia Pacific’s regional TV series The Greenbelt Reports highlighted. Filmed at 12 locations in four Asian countries (India, Indonesia, Sri Lanka and Thailand) which were hardest hit by the Indian Ocean tsunami of December 2004, the series showcased Nature’s protection against disasters and climate change.
It covered three coastal ecosystems or ‘greenbelts’ — coral reefs, mangroves and sand reefs. Reporters and producers from TVE Asia Pacific journalistically investigated the state of greenbelts in South Asia and Southeast Asia by talking to researchers, activists and government officials. They also looked at efforts to balance conservation needs with socio-economic needs of coastal communities.
Here’s the overview documentary (additionally, there were 12 stand-alone short videos as well):
The Greenbelt Reports: Armed by Nature: Part 1 of 3
The Greenbelt Reports: Armed by Nature: Part 2 of 3
The Greenbelt Reports: Armed by Nature: Part 3 of 3