I am not a public health or environmental expert, but have long covered related topics as a science journalist.
Among my long-standing interests are the downstream health and environmental effects agrochemicals – both chemical fertilizers and farm chemicals applied against pests and weeds. Parallel to this, I have also been covering chronic kidney disease of uncertain aetiology (CKDu), a mysterious illness that has been affecting thousands of Lankan farmers for nearly 25 years.
A link between agrochemicals and CKDu is suspected, but not yet scientifically proven (even though environmentalists ask us to believe so). It is a current yet contentious topic, which I chose for my presentation to an international workshop on “Pesticides and Global Health: Research, Collaboration and Impact” held at the Department of Anthropology, University of Durham, UK, on 10 – 11 February 2015.
In my presentation, I explore the topic from the angle of public perceptions, which are largely shaped by what appears in the media. This has been problematic since mass kidney failure in Sri Lanka has been compounded by what I call a ‘mass media failure’.
Most of our media have failed to understand, analyse and report adequately on this public health emergency. Instead of helping affected people and policy makers to work out solutions, some journalists have become amplifiers of extreme activist positions. This has led to alarmism and policy confusion.
What is to be done? There are no short-cuts to the scientific investigation process which must follow – that means further research is needed to find definitive evidence for causative factors. That could take a while, given how people are exposed to multiple environmental, lifestyle and genetic factors.
But meanwhile, the welfare of those already affected by the disease and their families needs to receive greater public support. Environmentalists trying to score points from this tragedy overlook this vital humanitarian aspect.
A few excerpts from the presentation below. See full presentation above.
Advocacy journalism is fine; activist journalism is questionableWe need Lankan media to be more reflective, less accusatorySpare a thought for today’s policy-makers who must think and act on the run…
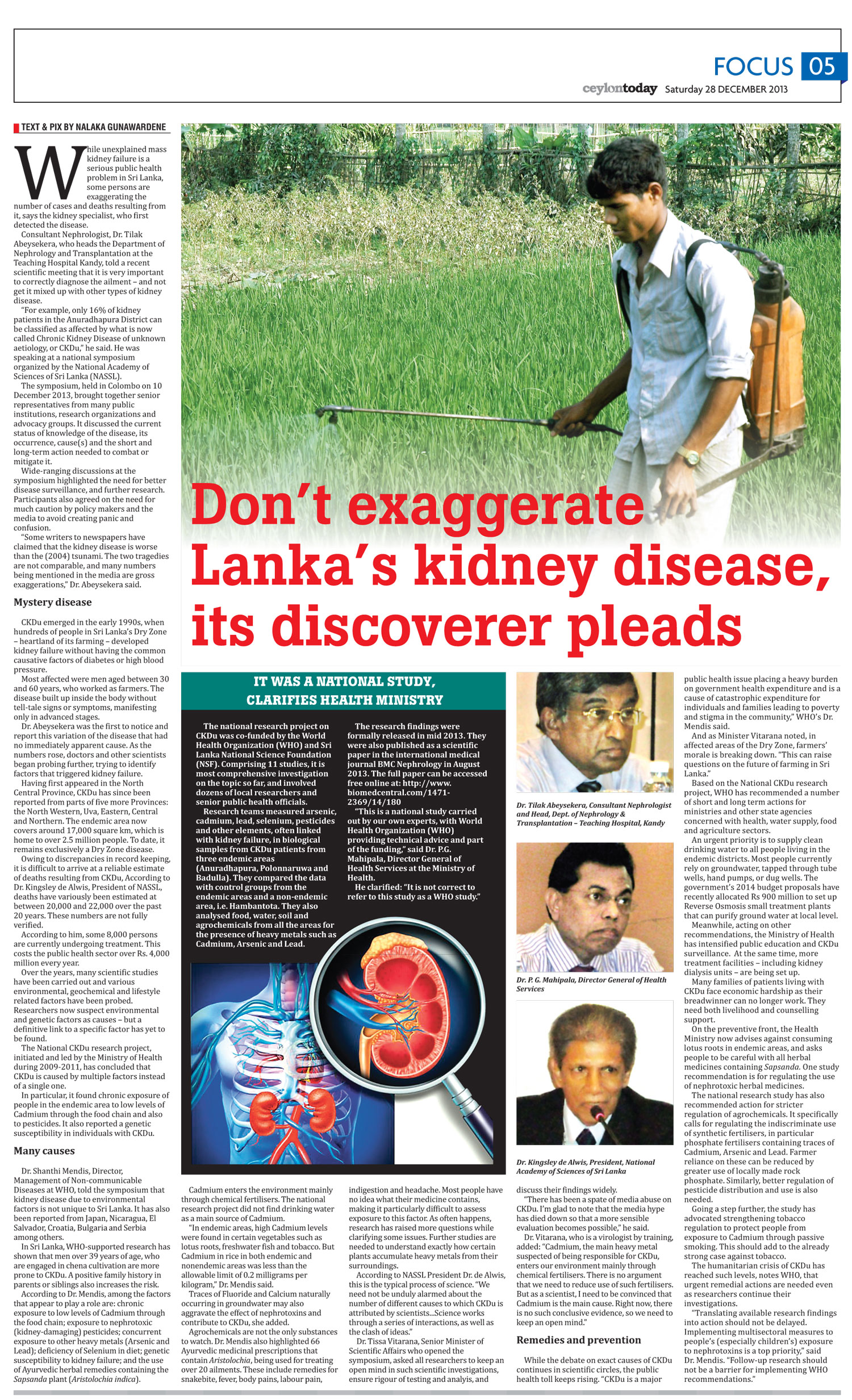
While unexplained mass kidney failure is a serious public health problem in Sri Lanka, some persons are exaggerating the number of cases and deaths resulting from it, says the kidney specialist who first detected the disease.
Consultant Nephrologist Dr Tilak Abeysekera, who heads the Department of Nephrology and Transplantation at the Teaching Hospital Kandy, told a recent scientific meeting that it is very important to correctly diagnose the ailment – and not get it mixed up with other types of kidney disease.
“For example, only 16% of kidney patients in the Anuradhapura district can be classified as affected by what is now called Chronic Kidney Disease of unknown aetiology, or CKDu,” he said. He was speaking at a national symposium organised by the National Academy of Sciences of Sri Lanka (NASSL).
The symposium, held in Colombo on 10 December 2013, brought together senior representatives from many public institutions, research organisations and advocacy groups. It discussed the current status of knowledge of the disease, its occurrence, cause(s) and the short and long-term action needed to combat or mitigate it.
Wide-ranging discussions at the symposium highlighted the need for better disease surveillance, and further research. Participants also agreed on the need for much caution by policy makers and the media to avoid creating panic and confusion.
“Some writers to newspapers have claimed that the kidney disease is worse than the (2004) tsunami. The two tragedies are not comparable, and many numbers being mentioned in the media are gross exaggerations,” Dr Abeysekera said.
Mystery disease
CKDu emerged in the early 1990s, when hundreds of people in Sri Lanka’s Dry Zone – heartland of its farming — developed kidney failure without having the common causative factors of diabetes or high blood pressure.
Most affected were men aged between 30 and 60 years who worked as farmers. The disease built up inside the body without tell-tale signs or symptoms, manifesting only in advanced stages.
Dr Abeysekera was the first to notice and report this variation of the disease that had no immediately apparent cause. As the numbers rose, doctors and other scientists began probing further, trying to identify factors that triggered kidney failure.
Having first appeared in the North Central Province, CKDu has since been reported from parts of five more provinces: the North Western, Uva, Eastern, Central and Northern. The endemic area now covers around 17,000 square km, which is home to over 2.5 million people. To date, it remains exclusively a Dry Zone disease.
Owing to discrepancies in record keeping, it is difficult to arrive at a reliable estimate of deaths resulting from CKDu, According to Dr. Kingsley de Alwis, President of NASSL, deaths have variously been estimated at between 20,000 and 22,000 over the past 20 years. These numbers are not fully verified.
According to him, some 8,000 persons are currently undergoing treatment. This costs the public health sector over Rs. 4,000 million every year.
Over the years, many scientific studies have been carried out and various environmental, geochemical and lifestyle related factors have been probed. Researchers now suspect environmental and genetic factors as causes – but a definitive link to a specific factor has yet to be found.
The National CKDu research project, initiated and led by the Ministry of Health during 2009-2011, has concluded that CKDu is caused by multiple factors instead of a single one (see also box below).
In particular, it found chronic exposure of people in the endemic area to low levels of Cadmium through the food chain and also to pesticides. It also reported a genetic susceptibility in individuals with CKDu.
Many causes
Dr Shanthi Mendis, Director, Management of Non-communicable Diseases at WHO, told the symposium that kidney disease due to environmental factors is not unique to Sri Lanka. It has also been reported from Japan, Nicaragua, El Salvador, Croatia, Bulgaria and Serbia among others.
In Sri Lanka, WHO-supported research has shown that men over 39 years of age who are engaged in chena cultivation are more prone to CKDu. A positive family history in parents or siblings also increases the risk.
According to Dr Mendis, among the factors that appear to play a role are: chronic exposure to low levels of Cadmium through the food chain; exposure to nephrotoxic (kidney-damaging) pesticides; concurrent exposure to other heavy metals (Arsenic and Lead); deficiency of Selenium in diet; genetic susceptibility to kidney failure; and the use of Ayurvedic herbal remedies containing the Sapsanda plant (Aristolochia indica).
Cadmium enters the environment mainly through chemical fertilisers. The national research project did not find drinking water as a main source of Cadmium.
“In endemic areas, high Cadmium levels were found in certain vegetables such as lotus roots, freshwater fish and tobacco. But Cadmium in rice in both endemic and nonendemic areas was less than the allowable limit of 0.2 milligrams per kilogram,” Dr Mendis said.
Traces of Fluoride and Calcium naturally occurring in groundwater may also aggravate the effect of nephrotoxins and contribute to CKDu, she added.
Agrochemicals are not the only substances to watch. Dr Mendis also highlighted 66 Ayurvedic medicinal prescriptions that contain Aristolochia, being used for treating over 20 ailments. These include remedies for snakebite, fever, body pains, labour pain, indigestion and headache. Most people have no idea what their medicine contains, making it particularly difficult to assess exposure to this factor.
As often happens, research has raised more questions while clarifying some issues. Further studies are needed to understand exactly how certain plants accumulate heavy metals from their surroundings.
According to NASSL President Dr de Alwis, this is the typical process of science. “We need not be unduly alarmed about the number of different causes to which CKDu is attributed by scientists…Science works through a series of interactions, as well as the clash of ideas.”
Dr Tissa Vitarana, Senior Minister of Scientific Affairs who opened the symposium, asked all researchers to keep an open mind in such scientific investigations, ensure rigour of testing and analyis, and discuss their findings widely.
“There has been a spate of media abuse on CKDu. I’m glad to note that the media hype has died down so that a more sensible evaluation becomes possible,” he said.
Dr Vitarana, who is a virologist by training, added: “Cadmium, the main heavy metal suspected of being responsible for CKDu, enters our environment mainly through chemical fertilisers. There is no argument that we need to reduce use of such fertilisers. But as a scientist, I need to be convinced that Cadmium is the main cause. Right now, there is no such conclusive evidence, so we need to keep an open mind.”
Remedies & prevention
While the debate on exact causes of CKDu continues in scientific circles, the public health toll keeps rising.
“CKDu is a major public health issue placing a heavy burden on Government health expenditure and is a cause of catastrophic expenditure for individuals and families leading to poverty and stigma in the community,” WHO’s Dr Mendis said.
And as Minister Vitarana noted, in affected areas of the Dry Zone, farmers’ morale is breaking down. “This can raise questions on the future of farming in Sri Lanka.”
Based on the National CKDu research project, WHO has recommended a number of short and long term actions for ministries and other state agencies concerned with health, water supply, food and agriculture sectors.
An urgent priority is to supply clean drinking water to all people living in the endemic districts. Most people currently rely on groundwater, tapped through tube wells, hand pumps, or dug wells. The government’s 2014 budget proposals have recently allocated Rs 900 million to set up Reverse Osmosis small treatment plants that can purify ground water at local level.
Meanwhile, acting on other recommendations, the Ministry of Health has intensified public education and CKDu surveillance. At the same time, more treatment facilities – including kidney dialysis units – are being set up.
Many families of patients living with CKDu face economic hardship as their breadwinner can no longer work. They need both livelihood and counselling support.
On the preventive front, the Health Ministry now advises against consuming lotus roots in endemic areas, and asks people to be careful with all herbal medicines containing Sapsanda. One study recommendation is for regulating the use of nephrotoxic herbal medicines.
The national research study has also recommended action for stricter regulation of agrochemicals. It specifically calls for regulating the indiscriminate use of synthetic fertilisers, in particular phosphate fertilisers containing traces of Cadmium, Arsenic and Lead. Farmer reliance on these can be reduced by greater use of locally made rock phosphate. Similarly, better regulation of pesticide distribution and use is also needed.
Going a step further, the study has advocated strengthening tobacco regulation to protect people from exposure to Cadmium through passive smoking. This should add to the already strong case against tobacco.
The humanitarian crisis of CKDu has reached such levels, notes WHO, that urgent remedial actions are needed even as researchers continue their investigations.
“Translating available research findings into action should not be delayed. Implementing multisectoral measures to people’s (especially children’s) exposure to nephrotoxins is a top priority,” said Dr Mendis. “Follow-up research should not be a barrier for implementing WHO recommendations.”
Text box:
It was a national study, clarifies Health Ministry
The national research project on CKDu was co-funded by the World Health Organization (WHO) and Sri Lanka National Science Foundation (NSF). Comprising 11 studies, it is most comprehensive investigation on the topic so far, and involved dozens of local researchers and senior public health officials.
Research teams measured arsenic, cadmium, lead, selenium, pesticides and other elements, often linked with kidney failure, in biological samples from CKDu patients from three endemic areas (Anuradhapura, Polonnaruwa and Badulla). They compared the data with control groups from the endemic areas and a non-endemic area, i.e. Hambantota. They also analysed food, water, soil and agrochemicals from all the areas for the presence of heavy metals such as Cadmium, Arsenic and Lead.
The research findings were formally released in mid 2013. They were also published as a scientific paper in the international medical journal BMC Nephrologyin August 2013. The full paper can be accessed free online at: http://www.biomedcentral.com/1471-2369/14/180
“This is a national study carried out by our own experts, with World Health Organization (WHO) providing technical advice and part of the funding,” said Dr P.G. Mahipala, Director General of Health Services at the Ministry of Health.
He clarified: “It is not correct to refer to this study as a WHO study.”
Don’t exaggerate Lanka’s kidney disease – by Nalaka Gunawardene – Ceylon Today, 28 Dec 2013
In Sri Lanka, mass kidney failure during the past two decades has been followed by what I call a mass media failure. Most of our media have failed to understand, analyse and report adequately on this public health emergency. Instead of helping affected people and policy makers to work out solutions, some journalists have become amplifiers of extreme activist positions.
I talked about this at at the International Science Communication Leadership Workshop, held as part of Association of Academies & Societies of Sciences in Asia (AASSA) General Assembly in Colombo, 16-19 October 2012. An English article based on my talk appeared in Ceylon Today a few days ago:
Mass Kidney Failure & Mass Media Failure: Go ‘Upstream’ for Remedies!
I have just written up similar views (NOT a translation!) for my weekend Sinhala language column in Ravaya broadsheet newspaper:
CKDu infographic courtesy Center for Public Integrity, USA
Ceylon Today newspaper has just published my article titled: Mass Kidney Failure & Mass Media Failure: Go ‘Upstream’ for Remedies!
It is adapted from a paper I presented last week at the International Science Communication Leadership Workshop, held as part of Association of Academies & Societies of Sciences in Asia (AASSA) General Assembly in Colombo, 16-19 October 2012.
In Sri Lanka, mass kidney failure during the past two decades has been followed by what I call a mass media failure. Most of our media have failed to understand, analyse and report adequately on this public health emergency. Instead of helping affected people and policy makers to work out solutions, some journalists have become amplifiers of extreme activist positions.
As health officials and policy makers struggle with the prolonged humanitarian crisis, partisan media coverage has added to public confusion, suspicion and fear. As a science writer and journalist, I have watched this with growing concern.
This is a critique of the Lankan media sector to which I have belonged, in one way or another, for a quarter century. I hope this will inspire some much-needed self-reflection among our media, which I feel over overstepped the boundaries of advocacy journalism in this issue. As I suggest, a return to first principles can help…
Full article below. Constructive engagement is welcomed.
Mass Kidney Failure & Mass Media Failure – Nalaka Gunawardene – Ceylon Today 25 Oct 2012
The kidneys are vital organs in our body that help keep the blood clean and chemically balanced through filtering. Healthy kidneys separate waste and excess water.
Similarly, a healthy and vibrant media helps separate fact from fiction, and provides clarity and context vital for an open, pluralistic society to function.
In Sri Lanka, mass kidney failure during the past two decades has been followed by what I see as a mass media failure to understand, analyse and report adequately on this public health emergency. Instead of helping affected people and policy makers to work out solutions, some journalists have become mere amplifiers of extreme activist positions.
As health officials and policy makers struggle with the prolonged humanitarian crisis, partisan media coverage has added to public confusion, suspicion and fear. As a science writer and journalist, I have watched this with growing concern.
I just gave a talk on this to the Science Communication Leadership Workshop which was part of the First General Assembly of Association of Academies and Societies of Sciences in Asia (AASSA) held in Colombo, Sri Lanka, on 17 October 2012.