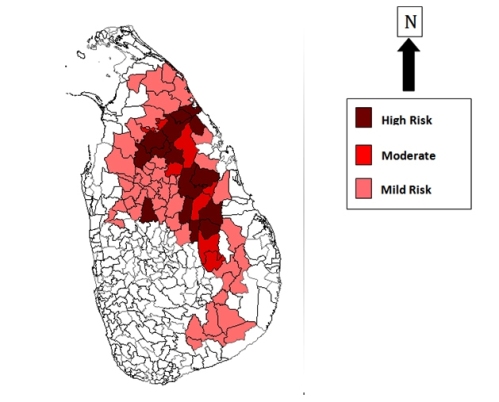
Beginning in the 1990s, thousands of people in Sri Lanka’s Dry Zone – heartland of its rice farming — developed kidney failure without having diabetes or high blood pressure, the common causative factors. Most affected were men aged 30 to 60 years, who worked as farmers. As numbers rose, puzzled doctors and other scientists started probing possible causes for what is now named Chronic Kidney Disease of unknown etiology (abbreviated as CKDu).
CKDu has become a fully-fledged public health crisis and humanitarian emergency, affecting thousands of people and their families – most of them subsistence farmers. Investigating causes of this ailment — still not pinned down to a specific cause or factor — has proven difficult. While scientists follow rigorous scientific methods, some ultra-nationalists and opportunistic politicians are trying to hijack the issue for their own agenda setting.
Sadly, some journalists and media outlets have added fuel to the fire with sensationalist reporting and unwarranted fear-mongering. For several years, I have documented the kind of misinformation, myths and pseudo-science uncritically peddled by Lankan media on CKDu.
In late 2012, speaking at an Asian science communication workshop held in Colombo, I first coined the phrase: Mass Media Failure is complicating Mass Kidney Failure. In December 2015, I revisited and updated this analysis, arguing that there are many reasons for systemic media failure in Sri Lanka that has allowed ultra-nationalists and certain environmental activists to pollute the public mind with half-truths and conspiracy theories. These need media industry level reform. Meanwhile, for improving the CKDu information flow in society, I proposed some short, medium and long term recommendations.
This article was written in December 2016 at the invitation of the Presidential Task Force on Prevention of Chronic Kidney Disease, to be included in a book the Presidential Secretariat was compiling.
හේතු හඳුනා නොගත් වකුගඩු රෝගය (Chronic Kidney Disease of uncertain aetiology, CKDu) ජාතික ආපදාවක්. මානුෂික ඛේදවාචකයක්. මේ ගැන මීට වඩා පුළුල් හා ප්රශස්ත ලෙසින් සමස්ත ලක් සමාජයේ අවධානය අවශ්යයි.
නගර කේන්ද්රීය වූ අපේ ජනමාධ්යවලට CKDu රෝගය හරිහැටි ග්රහණය කර ගැනීමටත් වසර කිහිපයක් ගත වුණා. මන්ද රෝගය මතු වී පැතිර ගියේ අගනුවරට දුරින් වියලි කලාපයේ නිසා.
දැන් මෙය නිතර පුවත් මවන මතෘකාවක් වුවත් බොහෝ වාර්තාකරණයන් කැරෙන්නේ ආවේගශීලී ලෙසින්. රජයට, සෞඛ්ය බලධාරීන්ට චෝදනාත්මක ස්වරයෙන්.
වකුගඩු රෝගය ගැන මහජනයාගේ හා ප්රතිපත්ති සම්පාදකයන්ගේ නිසි අවධානය යොමු කිරීමට මාධ්ය වාර්තාකරණයට විශාල මෙහෙවරක් කළ හැකියි. එහෙත් සමහර මාධ්යවේදීන් හෝ පරිසරවේදීන් බලාපොරොත්තු වන මට්ටමේ සරල හා ක්ෂණික විසඳුම් දීම නම් ප්රායෝගික නැහැ.
මේ රෝගය මතුව ඇත්තේ ශ්රී ලංකාවේ පමණක් නොවේ. ඉන්දියාවේ ආන්ද්රා ප්රදේශ් ප්රාන්තයේත්, මෙක්සිකෝව, ග්වාතමාලාව, එල්සැල්වදෝරය, නිකරගුවා, හොන්ඩුරාස් හා කොස්ටාරිකා යන ලතින් අමෙරිකානු රටවලත්, ඊජිප්තුවේත් මෙයට සමාන රෝග තත්ත්ව හමු වනවා.
මේ සියළු රටවල සෞඛ්ය බලධාරීන්ට තිබෙන ලොකුම අභියෝගය නම් විද්යාඥයන් හේතු සාධක සොයන අතරේ තිබෙන දැනුම යොදා ගෙන රෝගීන්ට ප්රතිකාර ලබාදීම හා එය හමු වන ප්රදේශවල අන් අයට රෝගයෙන් වැළකී සිටීමට දිය හැකි හොඳම උපදෙස් ලබා දීමයි.
හේතුකාරක තවමත් සොයනවා
ශ්රී ලංකාවේ 1990 දශකයේ උතුරුමැද පළාතේ මුල් වරට වාර්තා වූ මේ රෝගයට හේතු වන නිශ්චිත සාධකයක් තවමත් හඳුනා ගෙන නැහැ. මිනිස් සිරුර එක විට බොහෝ බලපෑම්වලට හසු වන නිසා එක් රෝගාබාධයකට තුඩු දෙන තනි සාධකයක් වෙන් කර ගැනීම විද්යාත්මකව ඉතා දුෂ්කරයි.
ගෙවී ගිය දශක දෙකකට වැඩි කාලයක් තුළ ජානමය, පාරිසරික හා ජීවන රටා ලෙස කාණ්ඩ කළ හැකි සාධක රැසක් විද්යාත්මක විමර්ශනයට ලක්ව තිබෙනවා.
රටේ සමහරක් ජනයාට මේ රෝගය හට ගැනීමට පාරම්පරිකව ලද ජානමය නැඹුරුවක් ඇත්දැයි පර්යේෂකයන් සොයා බලමින් සිටිනවා. මන්ද මේ රෝගය වාර්ත වී ඇත්තේ රටේ සමහර ප්රදේශවලින් පමණක් වීමයි.
ජීවන රටාව කාණ්ඩය යටතේ දුම්කොළ, මත්පැන් (විශේෂයෙන් කසිප්පු), ජලය ඇති තරම් නොබීම, දැඩි උණුසුමට ලක් වීම, එළිමහනේ දිගටම වැඩ කිරීම ආදි සාධක පර්යේෂකයන්ගේ විමසිල්ලට ලක් වනවා.
පාරිසරික සාධක කාණ්ඩය යටතේ භූගත ජලයේ ස්වාභාවිකවම හමු වන ෆ්ලෝරයිඩ්, වතුරෙහි කැල්සියම් වැනි ඛනිජ ස්වාභාවික මුසු වී තිබීම, මතුපිට ජලයේ බැක්ටීරියා ශ්රාවය කරන විස, බැර ලෝහ (කැඩ්මියම්, ආසනික්) ආහාරවල හෝ ජලයේ මුසු වීම ආදිය පර්යේෂණයට ලක්ව තිබෙනවා. මේ සමහරක් එන්නේ කෘෂි රසායනික (පොහොර, කෘමිනාශක, වල්නාශක) හරහා බවට කල්පිතයක් තිබෙනවා.
ජාත්යන්තරව පිළිගත් විද්වත් පර්යේෂන සඟරාවල පළ වූ නිබන්ධවලින් මේ දක්වා මෙවන් කල්පිත 30කට වඩා මතු කර තිබෙනවා. එකක්වත් තහවුරු වී නැහැ. ඒ සියල්ල තවමත් වැඩිදුර විවාදයට විවෘතයි. රෝගයට හේතුව එක සාධකයක් නොව සාධක කිහිපයක සංකලනයක් විය හැකි බවටත් අනුමාන කැරෙනවා.
විද්යාවේ ස්වභාවය පියවරෙන් පියවර, සාක්ෂි මත පදනම් වී, ආවේගශීලී නොවී දැනුම සොයා යාමයි. තිබෙන දැනුම ටිකෙන් ටික නිරවුල් කිරීමයි. එහෙත් වකුගඩු රෝගය ගැන සංවාදවලට කිරීමට යොමු වී සිටින සමහරුන්ට මෙසේ ක්රමානුකූලව ඉදිරියට යාමට ඉවසිල්ලක් නැහැ. ඔවුන් ප්රතිපත්ති සම්පාදකයන්ට බල කරන්නේ අනුමාන මත පදනම් වී යම් හදිසි හා ප්රබල පියවර ගන්නා ලෙසයි.
මෙවන් තත්ත්වයකදී යම් ආරක්ෂිත පියවර (precautionary measures) ගැනීම වැදගත්. තවත් ජනයා රෝගයට ලක් වීම හැකි නම් වළක්වා ගැනීම සඳහා. එහෙත් මේ ආපදාව නිමිත්ත කර ගෙන කෘෂි ප්රතිපත්තියේ හෝ ප්රතිපත්තිවල ප්රබල වෙනස්කම් කිරීම හා අනුමාන මත රාජ්ය ප්රතිපත්ති නිර්ණය කිරීම අවදානම් සහගත කාරියක්.
වසර 25කට වඩා මෙරට විද්යා මාධ්ය සන්නිවේදනයේ යෙදුනු අයකු ලෙස මගේ මතය නම් මෙවන් අවස්ථාවකදී මාධ්ය එක් මතවාදයකට පක්ෂග්රාහී නොවිය යුතු බවයි. පැත්තක් ගන්නට ඕනැම නම් රෝගයට ලක් වී පීඩාවට පත් අය හා ඔවුන්ගේ පවුල් වෙනුවන් හඬක් නැගීම කළ හැකියි.
බොරු භීතිය පතුරවන්න එපා!

පේරාදෙණිය ශික්ෂණ රෝහලේ වකුගඩු රෝග විශේෂඥ වෛද්ය තිලක් අබේසේකර විසින් CKDu මුල් වරට හඳුනා ගනු ලැබුවේ 1990 දශකයේදී. එතැන් පටන් වසර 20කට වැඩි කාලයක් පුරා මේ රෝගය හරිහැටි අවබෝධ කරගන්නට ඔහු තැත් කරනවා.
ඔහු අවධාරණය කරන මූලික කරුණක් නම් සමහර වකුගඩු රෝගීන්ගේ එයට තුඩු දෙන ශාරීරික සාධක හඳුනා ගත හැකි බවයි. මේ සාධක අතර දියවැඩියාව හා අධික රුධිර පීඩනය ප්රධානයි. මේ රෝග තත්ත්වයට CKD යයි කියනවා. එහි කිසිදු අබිරහසක් නැහැ.
CKD හරහා වකුගඩු අකරණයට ලක්වන යම් ජන පිරිසක් හැම රටකම හමු වනවා. හඳුනා ගන්නා විට පවතින තත්ත්වය අනුව බෙහෙත් මගින් හෝ රුධිර කාන්දු පෙරීම (dialysis) මගින් හෝ නිරෝගී වකුගඩුවක් බද්ධ කිරීමෙන් හෝ ප්රතිකාර කරනවා.
එහෙත් CKDu මීට වෙනස්. CKDu යනු විද්යාවෙන් දැනට හඳුනා ගත් ශාරීරික සාධක නැති පුද්ගලයන්ටද වකුගඩු අකරණය හට ගැනීමයි. එබැවින් ‘හේතු හඳුනා නොගත්’ යයි කියනවා.
මේ CKDu රෝගය මුලින් හමු වූ අනුරාධපුර දිස්ත්රික්කයේ වකුගඩු රෝගීන් සමස්තයෙන් 70%ක් පමණ CKDu. ඉතිරි 30% හේතු දන්නා වකගුඩු අකරණය හෙවත් CKD. මේ රෝග තත්ත්ව දෙක එකට මිශ්ර කිරීම හෝ පටලවා ගැනීම හෝ නොකළ යුතු බව වෛද්ය අබේසේකර කියනවා.
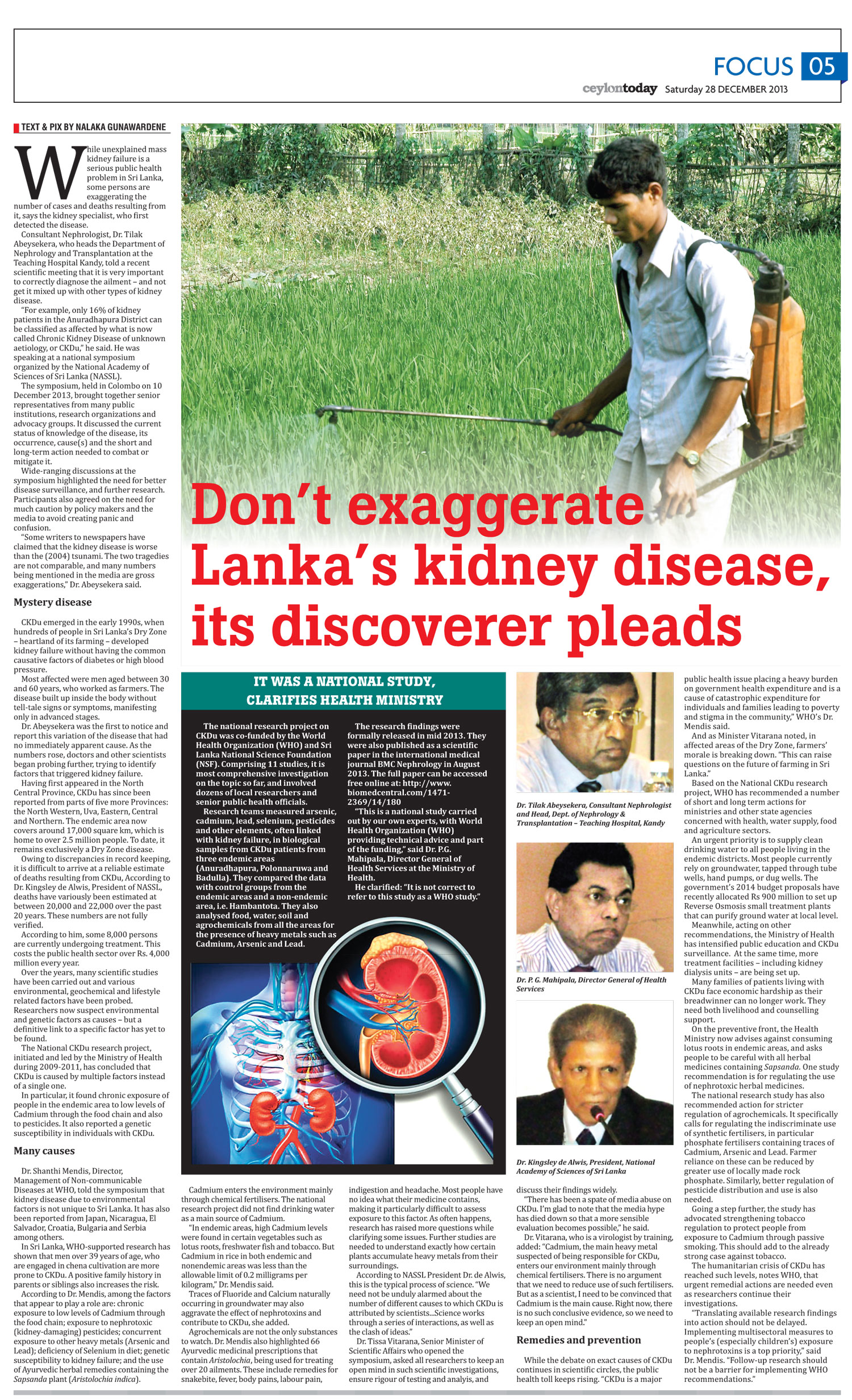
වෛද්ය අබේසේකර කියන්නේ පුවත්පත්වලට ලිපි ලියන ඇතැම් දෙනා මේ වෙනස නොදැන හෝ නොසලකා හැර හෝ තත්ත්වය සැබෑවට වඩා වැඩි කොට දක්වන බවයි.
‘‘සමහරු මෙය 2004 සුනාමියටත් වඩා බිහිසුණු යැයි කියනවා. මාධ්යවල මේ රෝගය ගැන සඳහන් කැරෙන බොහෝ සංඛ්යා ලේඛන අතිශයෝක්තීන්. මෙසේ කිරීමෙන් මේ රෝගය හරිහැටි තේරුම් ගැනීමට හා ප්රතිචාර දැක්වීමට වෛද්ය හා සෞඛ්ය බලධාරීන්ට තිබෙන අවකාශය ඇසිරෙනවා. රටේ හා සමාජයේ අනවශ්ය බියක් හා කලබලයක් ඇති කෙරෙනවා.”
එසේම CKDu ‘ශීඝ්රයෙන් පැතිරෙනවා’ වැනි ප්රකාශ කිරීමේදී ද ඉතා ප්රවේශම් විය යුතු යයි ඔහු කියනවා. මෙය රෝගියකුගෙන් තව කෙනෙකුට බෝවන ආකාරයේ රෝගයක් නොවෙයි.
‘‘අපට හරියටම කිව නොහැකියි මේ රෝගය පෙර තිබුනාට වඩා වැඩි දිස්ත්රික්ක ගණනකින් හඳුනා ගන්නේ එය වඩාත් දෙනකුට හට ගන්නා නිසාද නැතිනම් වැඩිපුර දෙනකු මෙය හට ගෙන ඇත්දැයි පරීක්ෂාවට ලක් වීම නිසාද කියා. සමහර විට ඇතැම් ප්රදේශවල රෝගීන්ද නොදැන මෙය වසර ගණනක් ඔවුන් තුළ කෙමෙන් හට ගනිමින් පැවතුණා විය හැකියි.”
CKDu රෝගයේ අදියර 5ක් තිබෙනවා. එයින් මුල් අදියර තුනේදීම රෝගියාට පෙනෙන හෝ දැනෙන රෝග ලක්ෂණ නැහැ. එය සොයා ගත හැක්කේ රුධිර හා මුත්රා සාම්පල් රසායනාගාර පරීක්ෂණවලින් පමණයි.
රෝග ලක්ෂණ පහළවන විට වකුගඩු සෑහෙන පමණට හානි වෙලා. එවිට කළ හැක්කේ බෙහෙත් හා රුධිර කාන්දු පෙරණය හරහා යම් තාක් කාලයක් ජීවත් වීමට රෝගියාට ඉඩ සලසා දීම පමණයි. මෙය පාලනය කරගත හැකි වුවත් සුව කළ හැකි රෝගයක් නොවෙයි.
‘වකුගඩු රෝගය මාරාන්තිකයි’ වැනි ප්රකාශ හරහා ද සමාජය භීතියට පත් නොකරන්න යැයි වෛද්ය අබේසේකර මාධ්යවලින් අයැද සිටිනවා. ‘සුව කළ නොහැකි වුව පාලනය කර ගන්නා දියවැඩියාව වැනි රෝග ගැන සමාජ ආකල්පය මීට වඩා බෙහෙවින් වෙනස්. ඇත්තටම නිරෝගී වකුගඩුවක් බද්ධ කළොත් CKD/CKDu රෝගින්ට දිගු කලක් ජීවත්වීමට ද හැකි වනවා.’
රෝගීන්ට සමාජ සත්කාරය
CKDu සෙමෙන් දිග හැරෙන මානුෂික ඛේදවාචකයක්. වෙනත් ආපදාවලදී මෙන් එක්වර ඇස හා මනස කම්පා කරවන ආකාරයේ ඡායාරූප හෝ විඩියෝ දර්ශන ජනිත කරන්නේ නැහැ.
රෝගය හමු වන ප්රදේශවල බිමෙහි හෝ අවට පරිසරයෙහි බැලූ බැල්මට වෙනසක් පෙනෙන්නේ නැහැ. හානිය වන්නේ මිනිසුන්ට, ගැහණුන්ට හා ඔවුන්ගේ පවුල්වලට පමණයි.
මේ ව්යසනයට මුහුණ දී සිටින පවුල් දහස් ගණනක් සිටිනවා. මෙයට ප්රතිචාර දැක්වීම හා රෝගීන් රැක බලා ගැනීම හුදෙක් රජයට පමණක් කළ හැකි දෙයක් නොවෙයි. පෞද්ගලික අංශය, ස්වේච්ඡා ආයතන, මාධ්ය, විද්වත් කණ්ඩායම් ඇතුලූ සමාජයේ සැමට මෙම සුබසාධනයේ කොටස්කරුවන් විය හැකියි.
රෝගයට ලක් වූ පවුල් සාමාජිකයා බොහෝ විට පවුලේ ප්රධාන හෝ එකම ආදායම් උපදවන්නායි. මේ නිසා රෝගීන්ගේ පවුල් ආර්ථික වශයෙනුත්, ඉනික්බිති මානසිකව හා සමාජයීය ලෙසත් මහත් පීඩාවට පත්වනවා.
මේ ව්යසනයට මුහුණ දී සිටින පවුල් දහස් ගණනක් සිටිනවා. මෙයට ප්රතිචාර දැක්වීම හා රෝගීන් රැක බලා ගැනීම හුදෙක් රජයට පමණක් කළ හැකි දෙයක් නොවෙයි. පෞද්ගලික අංශය, ස්වේච්ඡා ආයතන, විද්වත් කණ්ඩායම් ඇතුළු සමාජයේ සැමට මෙම සුබසාධනයේ කොටස්කරුවන් විය හැකියි.
පර්යේෂකයන් රෝගයට හේතු සොයන අතරේ සෙසු සමාජයට කළ හැකි හා කළ යුතු බොහෝ පියවර තිබෙනවා. සමාජ ආර්ථික පැත්තෙන් මෙන්ම මානසික හා ආකල්පමය පැත්තෙන් ද රෝගයට ලක් වූ අයගේ පවුල්වලට සමාජයේ කාරුණික උපකාර අවශ්යයි.
උදාහරණයකට මේ රෝගයට පානීය ජලය සම්බන්ධ යැයි සැක කැරෙනවා. රෝගය පවතින සියලුම දිස්ත්රික්කවල සැමට පානයට හිතකර පවිත්ර ජලය ලබා දීම අවශ්යයි. ජාතික ජල සම්පාදන හා ජලාපවාහන මණ්ඩලය මේ ලොකු වගකීම භාර ගෙන තිබෙනවා. ස්වේච්ඡා ආයතනවලටද මේ කාරියෙහි කොටස්කරුවන් විය හැකියි.
ගංවතුර, නායයාම් හා සුනාමි වැනි ආපදා සිදු වූ පසු ආධාර එකතු කිරීමට යොමු වන පිරිස සමග සසඳන විට මේ රෝගීන්ට පිහිට වන්නට පෙරට විත් තිබෙන්නේ සාපේක්ෂව ටික දෙනයි. ‘මාරාන්තික’ වකුගඩු රෝගය ගැන මොර දෙන මාධ්ය පවා රෝගයෙන් පීඩිත අයට ප්රායෝගිකව පිහිට වන්නේ කලාතුරකින්.
රෝග හේතුකාරක ගැන දිගටම කථා කරන අතරේ, වාද පිටියෙන් ඔබ්බට ගොස් මාධ්යවලට කළ හැකි මෙහෙවරක් තිබෙනවා. රාජ්ය හා ස්වේච්ඡා ආයතන නිහඬව කරන CKDu මානුෂික මෙහෙයුම් ගැනද මාධ්ය අවධානය මීට වඩා යොමු කළ යුතුයි.
රෝගීන් සිටින පවුල්වල ආත්ම අභිමානය පවත්වා ගනිමින් ඔවුන්ට ආර්ථික උදවු මෙන්ම මානසිකව ඔවුන්ට දිරියක් වීමත් අවශ්යයි.
සර්වෝදය මහ ලේකම් වෛද්ය වින්යා ආරියරත්න කියන්නේ මෙයයි: ‘රෝග කාරක හරියටම නිර්ණය කැරෙන තුරු බලා සිටීමට අපට බැහැ. අවශ්යත් නැහැ. නිශ්චිත රෝග කාරක සාධකය නොදැන අප ප්රතිචාර දක්වන තවත් රෝගාබාධ තිබෙනවා. (පිළිකා හා දියවැඩියාව වැනි). මේ නිසා පර්යේෂණ ඉදිරියට යන අතරේ අප සමාජයක් ලෙස මේ රෝගයෙන් පීඩාවට පත් අපේම සහෝදර ජනයා වෙනුවෙන් පෙළ ගැසෙමු. අපට ඔවුන්ගේ දුක හා දුෂ්කරතා අඩු කරන්නට හැකි අවස්ථා සොයා ඒ ඔස්සේ ඉදිරියට යමු.’
ඔහුගේ අදහස නම් 2004 සුනාමිය වෙරළබඩ බොහෝ ගම් නගරවලට හානි කළ විට රටක් හා සමාජයක් ලෙස එයට අප ප්රතිචාර දැක් වූවාට සමාන්තර ආකාරයේ දැවැන්ත කැප වීමක් වකුගඩු රෝගය සම්බන්ධයෙන් ද ඕනෑ බවයි.
උතුරුමැද පළාතේ රුධිර කාන්දු පෙරීම සඳහා පැමිණෙන රෝගීන්ගේ භාවිතය පිණිස සර්වෝදය හා මියුසියස් විදුහලේ බාලදක්ෂිකාවන් 2015දී අනුරාධපුරයේ ඉදි කළ ‘සුවෝදය’ නිවහන ඔහු උදාහරණයක් ලෙස සඳහන් කරනවා. මෙවැනි සමාජ සත්කාර අවස්ථා රාශියක් තිබෙනවා. තවත් බොහෝ උදවු අවශ්ය ද වනවා.
සංවේදී වාර්තාකරණය
නමුත් බොහොමයක් සමාජ සත්කාර ගැන මාධ්ය වාර්තාකරණයක් නෑ. සමාජ මාධ්ය ජාලවලින් (social media) නම් මේවා ගැන යම් කතාබහක් කැරෙනවා. ඒත් සමාජගත වනවා මදි.

මේ අතර සමාජ විද්යාඥයන් සොය ගෙන ඇත්තේ රෝගියකු සිටින පවුල් එම ප්රජාවේ කොන්කිරීමට (stigma) ලක් වන බවයි. ඒ පවුල්වලින් කසාදයක් පවා කර ගැනීමට මැලි වන තරමට මෙය දුර දිග ගිහින්. මෙය HIV ව්යාප්තියේ මුල් යුගයේ තිබූ සමාජ ප්රතිචාරයට සමාන්තර බව සමාජ විද්යාඥ ආචාර්ය කාලිංග ටියුඩර් සිල්වා පෙන්වා දෙනවා.
HIV මෙන්ම CKDu අරභයාත් මෙය අනියත බියක්. එය දුරු කිරීමට සංවේදී හා සානුකම්පිත මාධ්ය වාර්තාකරණයට ලොකු මෙහෙයක් කළ හැකියි.
මේ මානුෂික ප්රශ්නය තමන්ගේ පටු න්යායපත්රවලට අමතර තර්කයක් බවට හරවා ගත් සමහර අන්තවාදී පරිසරවේදීන් හා දේශපාලන ක්රියාකාරිකයන් ද සිටිනවා. ඔවුන්ගේ ප්රකාශ හා උද්ඝෝෂණ නිසා මේ අභියෝගය හරිහැටි තේරුම් ගෙන එයට ප්රතිචාර දැක්වීම ව්යාකූල වී තිබෙනවා.
උදාහරණයකට, සියලු කෘෂිරසායන භාවිතය එක් වරම නතර කිරීම සමහර හරිතවේදීන්ගේ දැඩි නිර්දේශයයි. පරිසර හිතකාමී ගොවිතැනකට කෙමෙන් අප යොමු විය යුතු නමුත් එය බලහත්කාරයෙන් හෝ කඩිමුඩියේ හෝ කළ හැකි දෙයක් නොවෙයි.
වකුගඩු රෝගය හා කෘෂිරසායන අතර මෙතෙක් හරිහැටි තහවුරු නොවූ සම්බන්ධය ගැන දිගටම වාද විවාද කිරීමට මාධ්ය නිසි වේදිකාවක් ලබා දිය යුතුයි. නැතිව අන්ත හරිතවාදීන්ට පමණක් ඉඩ දීම මාධ්යයේ වගකීම නොවෙයි.
ඒ අතර වකුගඩු රෝගීන්ගේ අවශ්යතා හා සුභසාධනයට මුල්තැන දෙන, එහෙත් ඔවුන්ගේ දුක විකුණා නොගන්නා සංවේදී හා සානුකම්පිත මාධ්යකරණයක් ඕනෑ.
ලේඛකයා ගැන: විද්යා ලේඛකයෙකු හැටියට වසර 25ක අධික කාලයක වෘත්තීය අත්දැකීම් ඇති නාලක ගුණවර්ධන පුවත්පත්, සඟරා, රේඩියෝ, ටෙලිවිෂන් හා ඉන්ටර්නෙට් යන සියලුම මාධ්ය හරහා සන්නිවේදනය කොට තිබෙනවා. එක් මාධ්යයකට, ආයතනයකට හෝ රටකට සීමා නොවී නිදහස් ලේඛකයෙකු ලෙස ඔහු දෙස් විදෙස් මාධ්ය හා පර්යේෂණ ආයතන සමඟ ක්රියා කරන්නේ විද්යාව, තාක්ෂණය හා සංවර්ධනය ගැන තොරතුරු සරලවත්, ආකර්ෂණීය ලෙසත් බෙදා හදා ගන්නටයි. 2011 පෙබරවාරියේ සිට රාවය පත්රයටට “සිවුමංසල කොලු ගැටයා” නමින් සතිපතා තීරු ලිපියක් ලියන නාලක, 2012 වසරේ විශිෂ්ඨතම තීරුලිපි රචකයා ලෙස විද්යොදය සාහිත්ය සම්මානයක් දිනා ගත්තා. ඔහුගේ ලිපි සියල්ල ඉන්ටර්නෙට් හරහා බලන්න: http://nalakagunawardene.com