http://ravaya.lk/?p=17269
The South-East Asia Region of the World Health Organization (WHO-SEARO) held its 69th Regional Committee meeting in Colombo from 5 to 9 September 2016. The meeting of 15 ministers of health from the region took a close look at Sri Lanka’s public health system – which has been able to provide substantial value over the decades.
Yet, the public health system rares gets the credit it deserves: the media and citizens alike often highlight its shortcomings without acknowledging what it delivers, year after year.
In this week’s Ravaya column (in Sinhala, appearing in the print issue of 4 Sep 2016), I salute the public health system of Sri Lanka that has accomplished much amidst various challenges.
Sri Lanka’s public hospitals and related field programmes – like public health inspectors, family health workers and specific disease control efforts — provide a broad range of preventive and curative services. In most cases, these are provided free to recipients, irrespective of their ability to pay.
This is sustained by taxes: Sri Lanka’s public health sector annually receives allocations equal to around 2% of the country’s GDP.
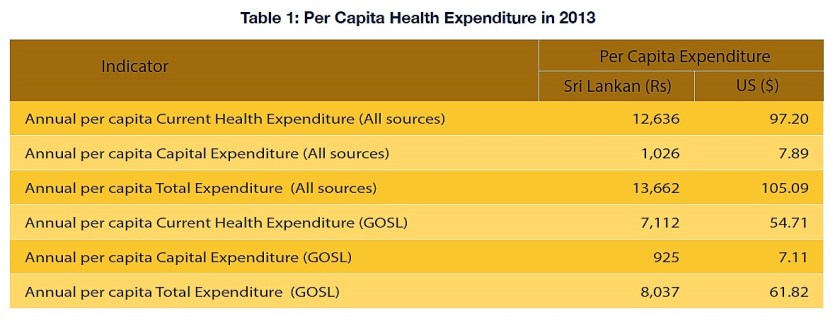
I quote from the recently released Sri Lanka National Health Accounts (2013) report. Its data analysis shows that the Government of Sri Lanka accounts for 55% of the total health care provision of the country. Considering all financial sources (public and private), the per capita current health expenditure of Sri Lanka in 2013 amounted to LKR 12,636 (97.2 US$).
![L to R - Dr Palitha Mahipala, Director General of Health Services, and Dr Jacob Kumaresan, WHO Representative to Sri lanka [WHO Photo]](https://nalakagunawardene.com/wp-content/uploads/2016/10/l-to-r-dr-palitha-mahipala-director-general-of-health-services-and-dr-jacob-kumaresan-who-representative-to-sri-lanka.jpg?w=840)
බැනුම් අසමින්, පම්පෝරිවලින් තොරව නිහඬව ලොකු වැඩ කරන මේ සේවය එළඹෙන සතියේ ආසියානු කලාපීය අවධානයට හා ඇගැයීමට ලක් වනවා. ඒ ලෝක සෞඛ්ය සංවිධානයේ (WHO) අග්නිදිග ආසියාතික කලාපයේ රටවල් 11ක සෞඛ්ය අමාත්යවරුන් සැප්තැම්බර් 5-9 දිනවල ඔවුන්ගේ වාර්ෂික රැස්වීම කොළඹදී පවත්වන නිසයි.
ලක් රජය සාමාජිකත්වය දරන අන්තර් රාජ්ය සංවිධානයක් වන WHO මෙරට ක්රියාත්මකවීම ඇරඹුණේ 1952දී. එනම් අප එක්සත් ජාතීන්ගේ සාමාජිකත්වය ලබන්නටත් වසර තුනකට පෙර.
වසර 65ක පමණ කාලයක් තිස්සේ මෙරට සෞඛ්ය සේවා නගා සිටුවීමට තාක්ෂණික උපදෙස් දෙන මේ ආයතනයේ මෙරටින් බිහිවූ වෛද්ය විශේෂඥයන් ගණනාවක්ද සේවය කරනවා.
ආදර්ශමත් සෞඛ්ය සේවයක් ලෙස WHO අප රට හඳුනා ගන්නේ ඇයි?
ශ්රී ලංකාවේ දේශීය වෙදකම් හා ප්රතිකාරවලට දිගු ඉතිහාසයක් තිබෙනවා. මේ ගැන සංක්ෂිප්ත විස්තරයක් වෛද්ය සී. ජී. ඌරගොඩ 1987දී ලියූ ශ්රී ලංකාවේ වෛද්ය විද්යාවේ ඉතිහාසය නම් පොතෙහි හමු වනවා. goo.gl/qBwMP6
එම මූලාශ්රයට අනුව නූතන, බටහිර වෛද්ය විද්යාව මෙරට ස්ථාපිත වන්නේ ලන්දේසි හා බ්රිතාන්ය පාලන යුගවලයි. ස්වදේශිකයන්ට ක්රමවත් මහජන සෞඛ්ය සේවාවක් ලබා දීමේ ප්රතිපත්තිමය තීරණ රැසක් ගනු ලැබුවේ බ්රිතාන්ය පාලකයන් විසින්.
වෛද්ය පර්යේෂණ විධිමත් ලෙස ඇරඹුණේද 1800න් පසුවයි. සිවිල් වෛද්ය දෙපාර්තමේන්තුව ලෙස 1801දී ඇරඹි රාජ්ය ආයතනය සෞඛ්ය දෙපාර්තමේන්තුවේ පූර්වගාමියා ලෙස දැකිය හැකියි. වසූරියට එරෙහිව එන්නත් කිරීම 1802දී ඇරඹුනා.
ප්රාථමික සෞඛ්ය කටයුතු සඳහා සෞඛ්ය ඒකක පිහිටුවීම ඇරඹුණේ 1926දී කළුතරින්. අද වන විට සෞඛ්ය නිලධාරී හෙවත් MOH කාර්යාල බවට පරිණාමය වී ඇත්තේ මේවායි.
මහජන සෞඛ්ය සේවාව යනු විවිධ වෘත්තිකයන් හා සේවකයන් රාශියකින් සමන්විත, දැවැන්ත ආයතනික ව්යුහයක්. වෛද්යවරුන්, හෙද සේවකයන්, රසායනාගාර තාක්ෂණවේදීන්, පරිපාලකයන්, පවුල් සෞඛ්ය සේවිකාවන්, සහකාර වෛද්ය සේවා, විශේෂිත බෝවන රෝග මර්දන එකක (මැලේරියා, ඩෙංගු. HIV ආදී) වැනි බොහොමයක් එයට අයත්.
ලක් සමාජය නිරෝගීව පවත්වා ගන්නට සෞඛ්ය සේවාව ප්රතිකාර මට්ටමින් (curative) හා වළක්වා ගැනීමේ මට්ටමින් (preventive) දිවා රාත්රී කරන මහා ව්යායාමයට ඇති තරම් අගය කිරීමක් නොලැබෙන බව මගේ අදහසයි.
එසේම මේ සද්දන්තයාගේ ක්රියාකාරීත්වය ගැන ඇතුළත දැක්මකින් සමාජයට තතු හෙළි කරන පිරිස ද අල්පයි. කලක් සෞඛ්ය සේවයේ සිට විශ්රාමික වෛද්ය ආරියසේන යූ. ගමගේ ලියන පුවත්පත් ලිපි හා පොත් හරහා අපට යම් ඉඟියක් ලද හැකියි.
රටේ ආදායම් මට්ටමට වඩා ඉහළ සෞඛ්ය සේවා දර්ශකයන් ලබා ගැනීමට සියවස් දෙකකට වැඩි කාලයක් ලද රාජ්ය අනුග්රහය හා ප්රමුඛතාව දායක වී තිබෙනවා.
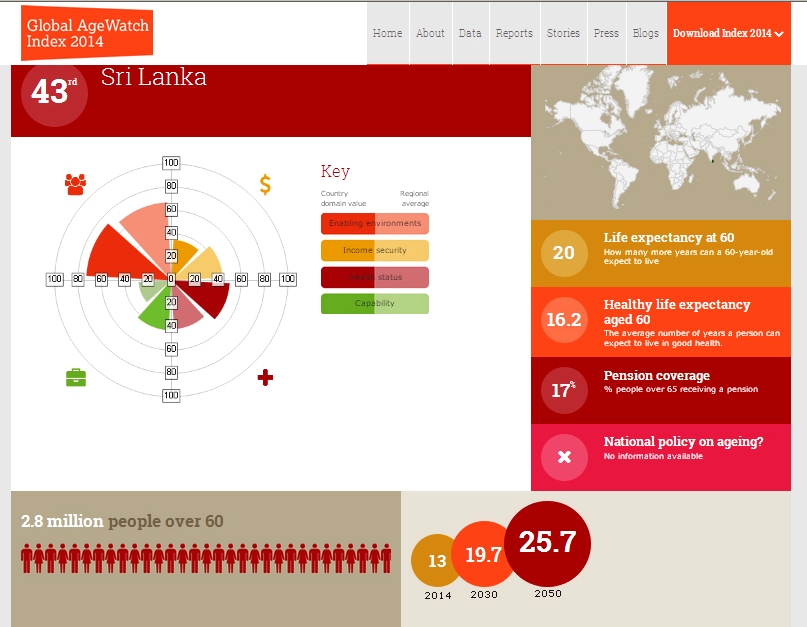
උදාහරණයකට 2012 වන විට අපේ රටේ වයස අවුරුද්දට අඩු ළදරු මරණ අනුපාතිකය සජීව උපත් 1,000කට 8යි. වයස 5ට අඩු ළමා මරණ අනුපාතිකය 12යි (2012). දරුවන් ලැබීම ආශ්රිතව සිදුවන මාතෘ මරණ සංඛ්යාව සජීව දරු උපත් ලක්ෂයකට 30යි.
මේ වන විට අපේ රටේ උපතේ දී අපේක්ෂා කළ හැකි ආයු කාලය පිරිමින්ට වසර 72ක්ද, ගැහැනුන්ට වසර 78.6ක්ද වනවා.
මෙකී නොකී මානව සංවර්ධන සාධක අතින් ශ්රී ලංකාව සිටින්නේ අපට වඩා වැඩි දළ ජාතික ආදායමක් ඇති බොහෝ රටවලට ඉදිරියෙන්.
එහෙත් සෞඛ්ය ක්ෂේත්රයේ අභියෝග කාලයත් සමග වෙනස් වනවා.
සමාජයක් ලෙස අපට තිබෙන ලොකු සෞඛ්ය අභියෝගයක් නම් ජීවත් වන කාලය තුළ හැකි තාක් දෙනෙකුට හැකි තාක් සෞඛ්යසම්පන්න, ඵලදායක ජීවන මට්ටම් ලබා දීමයි. වයස්ගත වීමේදී යම් අබල දුබලවීම් සිදුවීම ස්වාභාවික වුවත් නිදන්ගත රෝග හට ගැනීම අවම කර ගත යුතුව තිබෙනවා.
මෑතදී කොළඹ පැවති මාධ්ය හමුවකදී සෞඛ්ය සේවා අධ්යක්ෂ ජනරාල් වෛද්ය පාලිත මහීපාල අද ලක් සමාජය මුහුණදෙන සෞඛ්ය අභියෝග ගැන මනා විග්රහයක් කළා.
ඔහු කීවේ වත්මන් ශ්රී ලංකාව සංක්රාන්තීන් ගණනාවකට මැදිව සිටින බවයි.
- ජන විකාසමය සංක්රාන්තිය (demographic transition)( අති බහුතරයක් ළමයින් හා තරුණ තරුණියන්ගෙන් සමන්විතව තිබූ ජනසංයුතියක සිට අප කෙමෙන් මැදිවියේ හා වයස 60 ඉක්මවූවන් බහුතරයක් සිටින ජන සංයුතියකට යොමු වෙමින් සිටිනවා. 2012දී වයස 60ට වැඩි ප්රතිශතය 5%යි. 2031 වන විට මෙය 25%ක් වීමට ප්රක්ෂේපිතයිග මේ අයට බෝනොවන රෝග ඇතිවීමේ ප්රවණතාව වැඩියි.
- රෝග තත්ත්ව සංක්රාන්තිය (epidemiological transition)( බහුතරයක් රෝග තත්ත්ව (හා මරණ) බෝවන රෝග නිසා හට ගත් යුගයේ සිට සමාජය කෙමෙන් ගමන් කරන්නේ බහුතරයක් බෝ නොවන රෝග හටගැනීමටයි.
- පෝෂණ විද්යාත්මක සංක්රාන්තිය (nutritional transition)( කලකට පෙර වඩාත් සිරුරට හිතකර හා සමබර ආහාර ගත් අපේ ජනයාගේ ආහාර පරිභෝජන රටා ශීඝ්රයෙන් වෙනස් වෙමින් තිබෙනවා. දුවන ගමන් ගන්නා බොහෝ ආහාර දිගු කාලීනව අහිතකරයි. මේවා බෝ නොවන රෝගවලට දායක වනවා.
- ආර්ථීක සංක්රාන්තිය (economic transition): අඩු ආදායම්ලාභී රටක සිට මධ්යම ආදායම් ලබන රටක තත්ත්වයට අප පිවිස සිටිනවා. දුප්පත්කම මුළුමනින් තුරන් කර නැතත් මීට වසර 20කට පෙර තිබුණාට වඩා අද රටේ ජනයා අත මුදල් ගැවසෙනවා.
- ඩිජිටල් සංක්රාන්තිය (digital transition)( රටේ සමස්ත ජන සංඛ්යාව ඉක්මවා යන ජංගම දුරකතන සක්රිය ගිණුම් තිබෙනවා. විද්යුත් මාධ්ය විහිදයාමත් පුළුල්. මින් පෙර නොතිබූ ලෙස තොරතුරු ගලා යාමේ මාර්ග තිබෙනවා. ලෙඩරෝග හා ප්රතිකාර ගැන වැඩියෙන් දැන ගැනීම හරහා වඩාත් ඉහළ මට්ටමේ සෞඛ්ය සේවාවක් පුරවැසියෝ ඉල්ලා සිටිනවා.
මේ විග්රහයට මා මුළුමනින් එකඟයි. එයට තවත් එක් සංක්රාන්තියක් මා එකතු කරනවා. එනම් ජන ආකල්පමය සංක්රාන්තියයි (attitudinal transition).
දේශපාලකයන් හා නිලධාරීන් කියන දේ දොහොත් මුදුන් දී පිළිගෙන අනුගමනය කිරීමට අද පරපුර සූදානම් නැහැ. පෙරට වඩා බෙහෙවින් සංවාදශීලී — සමහර විට ආවේගශීලී — පොදු අවකාශයක් බිහි වෙමින් තිබෙනවා.
තවමත් දියුණු වෙමින් පවතින ශ්රී ලංකාව වැනි රටවල් මුහුණ දෙන ප්රධාන සෞඛ්ය සේවා අභියෝගයක් ද්විත්ව බර ඉසිලීමක් හෙවත් Double Burden ලෙස හැඳින් වෙනවා.
එහි සරල අරුත නම් නැතිබැරිකම් නිසා වැඩිපුරම හට ගන්නා, වළක්වා ගත හැකි බෝවන රෝග එක් පසෙකිනුත්, සාපේක්ෂව වඩාත් ඉසුරුබර ජීවන රටා නිසා හට ගන්නා බෝ නොවන රෝග තවත් පසෙකිනුත් එක වර දරා ගන්නට සෞඛ්ය සේවයට සිදු වීමයි.

බෝ නොවන රෝග වර්ග (Non-communicable Diseases, NCD) මූලික වශයෙන් ප්රභේද හතරක් තිබෙනවා: හෘදය රෝග හෙවත් කන්තු-වාහිනී ආබාධ (cardiovascular diseases) මුල් තැන ගන්නවා. ඊළඟට පිළිකා රෝගත්, ඉන් පසුව ශ්වසනාබාධ හා දියවැඩියාවත් මිලියන ගණන් ජනයාගේ සෞඛ්ය තත්ත්වය දුර්වල කරනවා. අකාලයේ මිය යෑමට හේතු වනවා.
මේ ද්විත්ව බර ගැන මා මුල් වරට විද්යා ලිපියක සාකච්ඡා කළේ 1999දී. (Sri Lanka’s Double Burden kills Rich and Poor Alike, May1999). ඒ සඳහා මා උපුටා දැක්වූ එක් විද්වතකු වූයේ ධූලකවේදය පිළිබඳ මහාචාර්ය වෛද්ය රවීන්ද්ර ප්රනාන්දුයි.
1990 දශකයේ සෞඛ්ය සංඛ්යා ලේඛන විග්රහ කරමින් ඔහු කීවේ ප්රජා සෞඛ්ය සේවා සඳහා එවකට වියදම් කරනු ලැබුවේ සමස්ත සෞඛ්ය ප්රතිපාදනවලින් 17%ක් පමණක් බවයි. එහෙත් බෝවන රෝග මෙන්ම බෝ නොවන රෝග ද වළක්වා ගැනීමේ ලොකුම විභවය ඇත්තේ ප්රජා මට්ටමින් ජනයා දැනුවත් කිරීම හරහායි.
‘ශ්රී ලංකාවේ අපේක්ෂා කළ හැකි ආයු කාලයන් දිගු වීම සෞඛ්ය සේවාවන්හි දිගු කාලීන ප්රතිඵලයක්. එහෙත් ප්රමාද වී මරණයට පත් වීම සැබෑ ජයග්රහණයක් වන්නේ ජීවත් වන කාලයේ යහපත් සෞඛ්යයෙන් සිටියහොත් පමණයි’ ඔහු පැහැදිලි කළා.
ජීවන රටා හා නොයෙක් පුරුදු හරහා දිගු කාලීනව හට ගන්නා බෝ නොවන නිදන්ගත රෝගාබාධ මතුවීමේ ඉඩකඩ වැඩියෙන් ඇත්තේ වයස්ගත වන විටයි. එහෙත් සමහර බෝ නොවන රෝග දැන් තරුණයන්ට හා ළමුන්ටද හට ගැනීම නිසා සෞඛ්ය සේවාවන්ට ලොකු පීඩනයක් ඇති කරනවා.
2016දීද අපේ සෞඛ්ය සේවාවට ද්විත්ව බර තවමත් බලපාන බව වෛද්ය මහීපාල කියනවා. එහෙත් ඒ බර දරමින්ම මහජන සෞඛ්ය ජයග්රහණයන් ලබා ගෙන තිබෙනවා.
සෞඛ්ය ක්ෂේත්රයේ නිතිපතා දත්ත කන්දරාවක් එකතු කැරෙනවා. වාර්ෂිකව සෞඛ්ය දත්ත වාර්තාවක් නිකුත් කරනවා. සෞඛ්ය අමාත්යාංශයේ වෙබ් අඩවියෙන් එය ලද හැකියි.
Sri Lanka Annual Health Bulletins http://www.health.gov.lk/moh_final/english/others.php?pid=110
එයට අමතරව සෞඛ්ය සේවා වියහියදම් විශ්ලේෂණය කරන ජාතික සෞඛ්ය මූල්ය වාර්තාවක්ද සම්පාදනය කරනවා : (Sri Lanka National Health Accounts).
මෑතදී නිකුත් වූ 2013 සෞඛ්ය මූල්ය වාර්තාවට අනුව එම වසරේ සෞඛ්ය ක්ෂේත්රය වෙනුවෙන් මෙරට වියදම් කරන ලද සමස්ත මුදල රුපියල් බිලියන් 281ක්. (ප්රාග්ධන ආයෝජන බිලියන් 21ක් හා පුනරාවර්තන වියදම් බිලියන් 260ක් ඇතුළත්.) මේ සමස්තය රටේ දළ ජාතික නිෂ්පාදිතයෙන් 3.2%ක් වනවා.
මේ කතා කරන්නේ රටේ සමස්ත සෞඛ්ය වියදම් ගැනයි. එයට රාජ්ය හා පෞද්ගලික දෙඅංශයේම සෞඛ්ය සේවා ඇතුළත්.
පුනරාවර්තන සෞඛ්ය වියදම් රු. බිලියන් 260න් සියයට 55%ක් රජය (එනම් මහජනයාගෙන්ම එකතු කර ගත් බදු මුදල්වලින්) දරන ලද අතර ඉතිරි 45% රක්ෂන ක්රම මගින්, සේව්යයන් විසින්, පුන්යායතන හරහා හෝ පුරවැසියන් ඍජුවම ගෙවා තිබෙනවා.
2013දී බෝ නොවන රෝග සඳහා සමස්ත සෞඛ්ය වියදමින් 35%ක් යොමු වී තිබෙනවා. බෝවන රෝග මර්දනයට හා ප්රතිකාරවලට 22%ක් වැය වුණා.
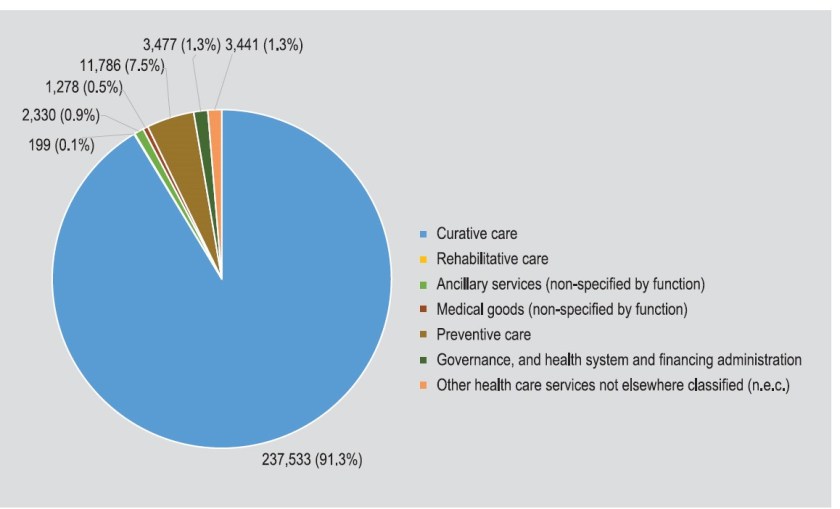
සාම්ප්රදායික හා විකල්ප ප්රතිකාර ක්රමවලට වැය කර ඇත්තේ බිලියන් 2.3ක් පමණයි. බහුතරයක් ප්රතිපාදන ලැබූ බටහිර වෛද්ය ක්රමයේ වුවද 91%ක් රෝග ප්රතිකාර සඳහා වැයවූ අතර වළක්වා ගැනීමට වැය කළේ 4.5%ක් පමණයි.
සෞඛ්ය සේවා සඳහා රජය වැය කරන ප්රමාණය දළ ජාතික නිෂ්පාදනයෙන් 2%ක් පමණ වනවා. මෙය ඉදිරි දෙවසර තුළ 3% දක්වා වැඩි කිරීමට රජයට වුවමනා බව වෛද්ය මහීපාල කියනවා.

2005-2016 අතර දශකය තුළ සෞඛ්ය ප්රතිපාදන 9 ගුණයකින් ඉහළ ගොස් ඇති බවත්, මහජන සෞඛ්ය සේවයේ ගුණාත්මක බව නැංවීම ප්රධාන ඉලක්කයක් බවත් ඔහු සඳහන් කළා.
සෞඛ්ය සේවාවේ අඩුපාඩු දකින්නෝ එහි ඵලදායීතාව ඇති තරම් නොදැකීම කනගාටුවට කරුණක්.
සෞඛ්යයට කරන සමස්ත වියදම සුවිසල් සේ පෙනුණත් 2013දී එක් පුරවැසියකුට කරන ලද සාමාන්ය වියදම රු. 12,636යි. අපට සමාන සෞඛ්ය දර්ශක ලබාගැනීම සඳහා වෙනත් බොහෝ රටවල මීට වඩා බෙහෙවින් වියදම් කරන බව වෛද්ය මහීපාල පෙන්වා දෙනවා.
රටේ පුනරාවර්තන සෞඛ්ය වියදමින් 24%ක්ම බෙහෙත්වලට වැය වීම අවධානයට ලක් විය යුත්තක්ග අත්යවශ්ය බෙහෙත් ප්රතිපත්තිය නිසි ලෙස ක්රියාත්මක කිරීමෙන් මෙය සීමා කර ගත හැකියි.
එසේම ඉදිරි වසරවලදී අධ්යාපනයට හා මහජන දැනුවත් කිරීම්වලට වැඩි ප්රමුඛත්වයක් දීම අවශ්යයි.
වැඩියෙන් රෝහල් ඉදි කර, නව තාක්ෂණය භාවිතයට ගත්තාට පමණක් මදි. ශාරීරික හා මානසික සුවතාවය රටේ සැමට ලබා දීමට තව කළ යුතු බොහෝ දේ තිබෙනවා. රජය හා සමාජය මේ වෙනුවන් අත්වැල් බැද ගත යුතුයි.