From that day, the island nation’s 21 million citizens can exercise their legal right to public information held by various layers and arms of government.
One month is too soon to know how this law is changing a society that has never been able to question their rulers – monarchs, colonials or elected governments – for 25 centuries. But early signs are encouraging.
Sri Lanka’s 22-year advocacy for RTI was led by journalists, lawyers, civil society activists and a few progressive politicians. If it wasn’t a very grassroots campaign, ordinary citizens are beginning to seize the opportunity now.
RTI can be assessed from its ‘supply side’ as well as the ‘demand side’. States are primarily responsible for supplying it, i.e. ensuring that all public authorities are prepared and able to respond to information requests. The demand side is left for citizens, who may act as individuals or in groups.
In Sri Lanka, both these sides are getting into speed, but it still is a bumpy road.
Cartoon by Gihan de Chickera, Daily Mirror
During February, we noticed uneven levels of RTI preparedness across the 52 government ministries, 82 departments, 386 state corporations and hundreds of other ‘public authorities’ covered by the RTI Act. After a six month preparatory phase, some institutions were ready to process citizen requests from Day One. But many were still confused, and a few even turned away early applicants.
Such teething problems are not surprising — turning the big ship of government takes time and effort. We can only hope that all public authorities, across central, provincial and local government, will soon be ready to deal with citizen information requests efficiently and courteously.
Some, like the independent Election Commission, have already set a standard for this by processing an early request for audited financial reports of all registered political parties for the past five years.
On the demand side, citizens from all walks of life have shown considerable enthusiasm. By late February, according to Dr Ranga Kalansooriya, Director General of the Department of Information, more than 1,500 citizen RTI requests had been received. How many of these requests will ultimately succeed, we have to wait and see.
Reports in the media and social media indicate that the early RTI requests cover a wide range of matters linked to private grievances or public interest.
Under the RTI law, public authorities can’t play hide and seek with citizens. They must provide written answers in 14 days, or seek an extension of another 21 days.
To improve their chances and avoid hassle, citizens should ask their questions as precisely as possible, and know the right public authority to lodge their requests. Civil society groups can train citizens on this, even as they file RTI requests of their own.
That too is happening, with trade unions, professional bodies and other NGOs making RTI requests in the public interest. Some of these ask inconvenient yet necessary questions, for example on key political leaders’ asset declarations, and an official assessment of the civil war’s human and property damage (done in 2013).
Politicians and officials are used to dodging such queries under various pretexts, but the right use of RTI law by determined citizens can press them to open up – or else.
The Right to Information Commission will play a decisive role in ensuring the law’s proper implementation. “These are early days for the Commission which is still operating in an interim capacity with a skeletal staff from temporary premises,” it said in a media statement on February 10.
The real proof of RTI – also a fundamental right added to Constitution in 2015 – will be in how much citizens use it to hold government accountable and to solve their pressing problems. Watch this space.
Science writer and media researcher Nalaka Gunawardene is active on Twitter as @NalakaG. Views in this post are his own.
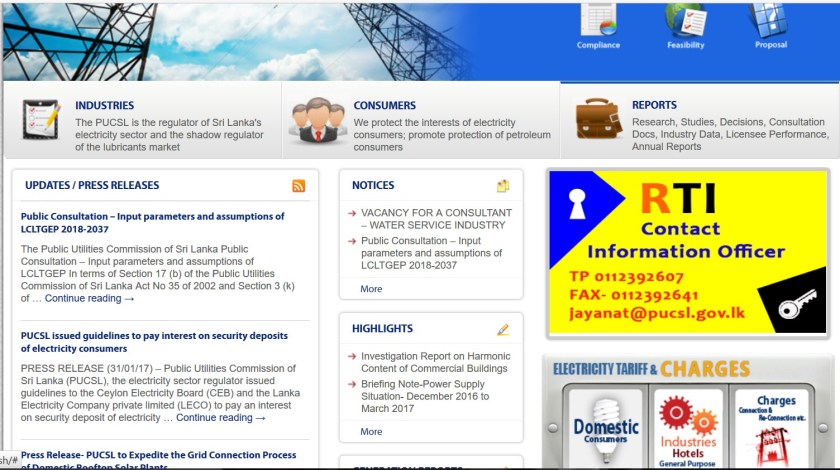
One by one, Sri Lanka public agencies are displaying their RTI officer details as required by law. Example: http://www.pucsl.gov.lk saved on 24 Feb 2017
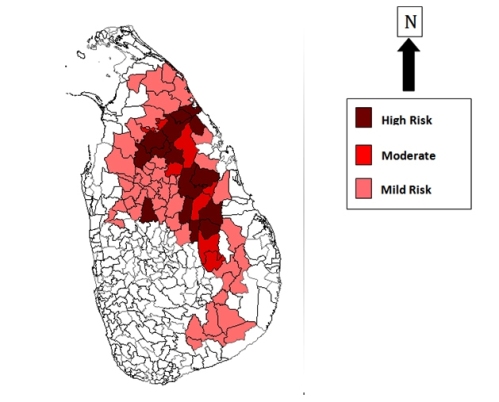
Image courtesy: Health Education Bureau, Ministry of Health, Sri Lanka
Beginning in the 1990s, thousands of people in Sri Lanka’s Dry Zone – heartland of its rice farming — developed kidney failure without having diabetes or high blood pressure, the common causative factors. Most affected were men aged 30 to 60 years, who worked as farmers. As numbers rose, puzzled doctors and other scientists started probing possible causes for what is now named Chronic Kidney Disease of unknown etiology (abbreviated as CKDu).
CKDu has become a fully-fledged public health crisis and humanitarian emergency, affecting thousands of people and their families – most of them subsistence farmers. Investigating causes of this ailment — still not pinned down to a specific cause or factor — has proven difficult. While scientists follow rigorous scientific methods, some ultra-nationalists and opportunistic politicians are trying to hijack the issue for their own agenda setting.
Sadly, some journalists and media outlets have added fuel to the fire with sensationalist reporting and unwarranted fear-mongering. For several years, I have documented the kind of misinformation, myths and pseudo-science uncritically peddled by Lankan media on CKDu.
In late 2012, speaking at an Asian science communication workshop held in Colombo, I first coined the phrase: Mass Media Failure is complicating Mass Kidney Failure. In December 2015, I revisited and updated this analysis, arguing that there are many reasons for systemic media failure in Sri Lanka that has allowed ultra-nationalists and certain environmental activists to pollute the public mind with half-truths and conspiracy theories. These need media industry level reform. Meanwhile, for improving the CKDu information flow in society, I proposed some short, medium and long term recommendations.
In this week’s Ravaya column (appearing in the print issue of 21 August 2016), I take a critical look at the Sri Lanka government’s new ‘Toxin-Free Nation” effort. Announced in 2015, it is a three year programme (2016-2018) “to convert Sri Lanka into a green nation and enable its citizens to enjoy foods free of chemicals and agro-toxins”.
Curiously, the programme is being implemented by a state entity called the Strategic Enterprise Management Agency (SEMA), set up in 2004 originally to monitor and support state owned enterprises. The century old and widely experienced Department of Agriculture is not involved (and apparently fully excluded).
Toxin free country – SEMA image
According to the official programme document, available on SEMA website, “the aim of the program is to replace import driven agrochemical based agriculture with organic, sustainable natural agro-culture.”
[Quoted verbatim: not sure why they insist on using the term agro-culture instead of agriculture.]
The document claims, without citing any references or sources, that Sri Lanka spends LKR 300 billion a year “to import milk products, sugar, agrochemicals, seeds, etc., while farmer subsidies account for a further Rs.30 billion a year” (p12).
It further says, on p23, “As a long-term strategy for toxin-free agriculture, it is anticipated that indigenous rice varieties will significantly replace the improved varieties that are presently grown by farmers. According to the plan, 30% of rice produced in Sri Lanka would be indigenous varieties at the end of the three year plan. Further, organic, natural, biological fertilizers and pest repellants will replace the agrochemicals used to cultivate these improved varieties and it is anticipated that these toxins will be completely eradicated from Sri Lankan soil by the third year of the program.”
The document is full of uncorroborated claims and seemingly unrealistic goals. In 2014, organically farmed land accounted for less than one percent of the total cultivated land in Sri Lanka.
The exact methodology of going from under 1 percent to 33% in three years is not clear. On p15, the document says: “A toxin-less agro-culture is a system geared to obtain the required “plant-food” from the air, the land and the immediate environment. Multicropping, soil conservation, water and irrigation management, promoting the presence of agrofriendly fauna and flora as well as mechanical systems for pest control are all part of these systems.”
The plan lists a 10 point, multi-pronged approach as follows:
The plan does make some sense when it takes stock of organically grown food available in the market today. “In 2015, the price of organics was two or three times that of foods produced with the application of agrochemicals. Therefore, only the middle upper and upper income bracket of consumer could afford them leaving the common citizen of the country no choice but to purchase and consume toxin laced alternatives.” (p13).
I have been saying this for years. As I wrote in August 2014: “Despite their appeal, organics will remain a niche market, albeit a growing one, for years to come. Nobody wants to eat food laced with agrochemical residues (for which no safe upper limits have been set in Sri Lanka). But when organics typically cost 50% or more than non-organics, how many can really afford it? Unless this gap is narrowed, organics will remain beyond reach for many.”
As a long standing watcher and commentator on conservation farming (which is bigger than organics), I have been seeking clarity on this Toxin-Free Nation plan of Sri Lanka, being spearheaded by President Maithripala Sirisena himself. But his staff involved in promoting and implementing the programme have opted not to respond to specific queries in the public media and scientific forums.
Worse, they have shown high levels of intolerance towards critics — sometimes vilifying critics as ‘agents of chemical farming’ or ‘promoters of agrochemical companies’! This utter failure to engage is inconsistent with good governance policies of the President and government. The Department of Agriculture being excluded from the whole process is also a matter for grave concern: this means there now are TWO parallel structures for farming policy and promotion in Sri Lanka!
In this column, I call for a dispassionate, rational discussion of this politically driven national programme for toxin-free farming. I also refer to three outstanding Lankan scientists who have advocated conservation farming for decades – but they have done so without the intellectual arrogance and confrontational politics of the current effort. These pathfinders are: late Dr Ray Wijewardene, Dr Lionel Weerakoon and Dr Parakrama Waidyanatha.
L to R – Dr Lionel Weerakoon, Dr Parakrama Waiyanatha, Asoka Abeygunawardena
Uncritical media reporting (such as this one in state media) leaves the Toxin-Free Nation Programme unchallenged even when its claims and plans don’t add up…
Image courtesy – Health Education Bureau of Sri Lanka
In this week’s Ravaya column (in Sinhala, published in issue dated 15 May 2016),, I revisit a public health emergency that I have been writing about for several years: mass kidney failure for no known reason.
Beginning in the 1990s, thousands of people in Sri Lanka’s Dry Zone – heartland of its rice farming — developed kidney failure without having diabetes or high blood pressure, the common causative factors. Most affected were men aged 30 to 60 years, who worked as farmers. As numbers rose, puzzled doctors and other scientists started probing possible causes for what is now named Chronic Kidney Disease of unknown etiology (abbreviated as CKDu).
CKDu has become a fully fledged humanitarian emergency, affecting thousands of people and their families – most of them subsistence farmers.
Investigating causes of this ailment — still not pinned down to a specific cause or factor — has proven difficult. While scientists follow rigorous scientific methods, some ultra-nationalists and opportunistic politicians are trying to hijack the issue for their own agenda setting. Some journalists have added fuel to the fire with sensationalist reporting and unwarranted fear-mongering.
On 9 May 2016, I moderated High Level Media Dialogue on Chronic Kidney Disease of Unknown Aetiology (CKDu) and Public Health in Colombo. It was organised jointly by the Ministry of Health, Nutrition and Indigenous Medicine; Ministry of Parliamentary Reforms and Mass Media; and theCoordinating Secretariat for Science, Technology and Innovation (COSTI) of the Ministry of Science, Technology and Research.
Three experienced medical professionals joined our conversation: Dr Tilak Abeysekera, Consultant Nephrologist, Nephrology Dialysis and Transplant Unit, General Hospital, Kandy; Dr Palitha Mahipala, Director General, Health Services, Ministry of Health, Nutrition and Indigenous Medicine; and Dr Vinya Ariyaratne, General Secretary of Sarvodaya and consultant community physician.
In this column, I summarise some of the latest scientific analysis and humanitarian issues that were presented during the event.
See also my other writing on the subject (some early ones are updated in this latest Ravaya column):
Science writer Nalaka Gunawardene speaks at National Policy Workshop on Prevention of Chronic Kidney Disease, held in Colombo on 16 Dec 2015
On 16 December 2015, I was invited by Sri Lanka’s Presidential Task Force for the Prevention of Chronic Kidney Disease to speak on this topic at the NATIONAL WORKSHOP ON PREVENTION OF CHORNIC KIDNEY DISEASE held in Colombo.
Speaking to an audience of scientists, health and agriculture sector public officials and policy makers, I briefly explored the kind of misinformation, myths and pseudo-science uncritically peddled by Lankan media.
Professor Rezvi Sheriff, Sri Lanka’s top kidney specialist, chairing National Policy Workshop on CKDu in Colombo, 16 Dec 2015
Scientists are researching widely on what causes the Chronic Kidney Disease of unknown etiology (CKDu) in Sri Lanka that affects thousands of people (mostly farm workers) and burdens the public healthcare system. As health officials and policy makers struggle with the prolonged humanitarian emergency, unprofessional and fear-mongering media coverage often adds to public confusion and fear.
As a science writer, I have long been concerned about public communication of risk in times of distress. In late 2012, speaking at an Asian science communication workshop held in Colombo, I first coined the phrase: Mass Media Failure is complicating Mass Kidney Failure.
I revisited and updated this analysis,arguing that there are many reasons for systemic media failure in Sri Lanka that has allowed ultra-nationalists and certain environmental activists to pollute the public mind with half-truths and conspiracy theories. These need media industry level reform.
Meanwhile, for improving the CKDu information flow in society, I proposed some short, medium and long term recommendations.
Text of my column written for Echelon monthly business magazine, Sri Lanka, July 2015 issue
Kidney Disease Needs ‘Heart and Mind’ solutions
By Nalaka Gunawardene
Mass kidney failure in Sri Lanka is a sign of wider systemic failure in land and water care
If bans and prohibitions were a measure of good governance, Sri Lanka would probably score well in global rankings. Successive governments have shown a penchant for banning – usually without much evidence or debate.
The latest such ban concerns glyphosate — the world’s most widely used herbicide – on the basis that it was causing chronic kidney disease in parts of the Dry Zone.
Then, on 29 May 2015, state-owned Daily News reported under Cabinet decisions: “The scientists who carry out research on renal diseases prevailing in many parts of the country have pointed out that the use of pesticides, weedicides and chemical fertiliser could be contributing to this situation. Accordingly the government has already banned the import and usage of four identified chemical fertilizer and pesticides. In addition to this President has decided to totally ban the import and usage of glyphosate.”
Has this decision tackled the massive public health and humanitarian crisis caused by mass kidney failure? Sadly, no. The new government has ignored the views of a vast majority of Lankan scientists, and sided with an unproven hypothesis. This undermines evidence-based policy making and allows activist rhetoric to decide affairs of the state.
The chronic kidney disease was first reported from certain parts of the Dry Zone in the early 1990s. Hundreds were diagnosed with kidney failure – but none had the common risk factors of diabetes, high blood pressure or obesity. Hence the official name: Chronic Kidney Disease of uncertain aetiology, or CKDu.
The disease built up stealthily in the body, manifesting only in advanced stages. By then, regular dialysis or transplants were the only treatment options. Most affected were male farmers in working age, between 30 and 60 years.
In early 2013, the Ministry of Health estimated that some 450,000 persons were affected. The cumulative death toll has been reported between 20,000 and 22,000, but these numbers are not verified.
The kidney specialist who first detected the disease worries that some activists are exaggerating CKDu numbers. Dr Tilak Abeysekera, who heads the department of nephrology and transplantation at the Kandy Teaching Hospital, underlines the critical need for correct diagnosis. CKDu should not be confused with regular types of kidney disease, he says.
It is clear, however, that CKDu has become a national humanitarian emergency. Providing medication and dialysis for those living with CKDu already costs more than 5% of the country’s annual health budget. With each dialysis session costing around LKR 12,000 (and 3 or 4 needed every week), very few among the affected can afford private healthcare.
Besides the mounting humanitarian cost, CKDu also has implications for agricultural productivity and rural economies as more farmers are stricken. With the cause as yet unknown (although confirmed as non-communicable), fears, myths and stigma are also spreading.
Looking for Causes
For two decades, researchers in Sri Lanka and their overseas collaborators have been investigating various environmental, geochemical and lifestyle-related factors. They have come up with a dozen hypotheses, none of it proven as yet.
Among the environmental factors suspected are: naturally high levels of Fluoride in groundwater; use of Aluminium utensils with such water; naturally occurring hard water (with high mineral content); cyanobacterial toxins in water; pesticide residues; and higher than safe levels of Cadmium or Arsenic. Lifestyle factors studied include the locally brewed liquor (kasippu), and certain Ayurvedic medicinal concoctions. Genetic predisposition to kidney failure has also been probed in some areas.
Researchers are baffled why CKDu is found only in certain areas of the Dry Zone when these environmental and lifestyle factors are common to a much larger segment of population. This makes it much harder to pinpoint a specific cause.
The most comprehensive study to date, the National CKDu Research Project (2009-2011), concluded that CKDu results from not one but several causes. The multidisciplinary study, led by Ministry of Health with support from the World Health Organisation (WHO), highlighted several risk factors. These include long-term exposure to low levels of cadmium and arsenic through the food chain, which are linked to the wide use of chemical fertilisers and pesticides. Selenium deficiency in the diet and genetic susceptibility might also play a part, the study found.
These findings were academically published in BMC Nephrology journal in August 2013 (See: www.biomedcentral.com/1471-2369/14/180). The paper ended with these words: “Steps are being taken to strengthen the water supply scheme in the endemic area as well as the regulations related to procurement and distribution of fertilizers and pesticides. Further studies are ongoing to investigate the contributory role of infections in the pathogenesis of CKDu.”
Hazards of Pseudoscience
One thing is clear. Remedial or precautionary measures cannot be delayed until a full understanding of the disease emerges. Indeed, WHO has recommended taking care of the affected while science takes its own course.
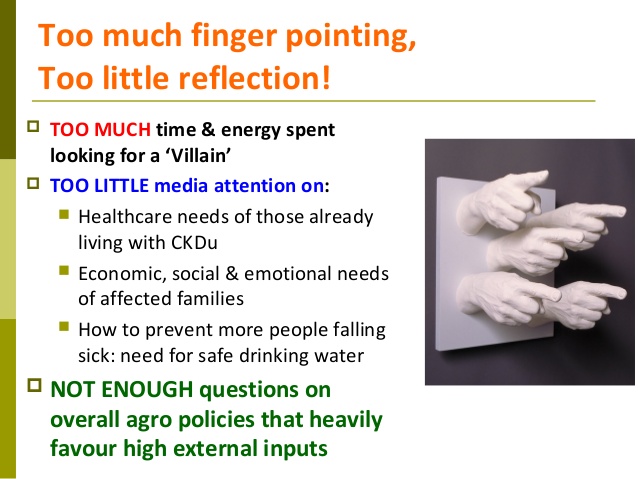
CKDu needs a well-coordinated response from public health, agriculture and water supply sectors that typically fall under separate government ministries and agencies. We need to see mass kidney failure as more than just a public health emergency or environmental crisis. It is a sign of cascading policy failures in land care, water management and farming over decades.
In such complex situations, looking for a single ‘villain’ is both simplistic and misleading. For sure, the double-edged legacy of the Green Revolution — which promoted high external inputs in agriculture — must be critiqued, and past policy blunders need correction. Yet knee-jerk reactions or patchy regulation can do more harm than good.
“In Sri Lanka we have a powerful lobby of pseudoscientists who seek cheap popularity by claiming to work against the multinational corporations for their own vested political interests,” says Dr Oliver A Ileperuma, a senior professor of chemistry at Peradeniya University. In his view, the recent glyphosate ban is a pure political decision without any scientific basis.
His concerns are shared by several hundred eminent Lankan scientists who are fellows of NASSL, an independent scientific body (not a state agency). The Academy said in a statement in mid June that it was “not aware of any scientific evidence from studies in Sri Lanka or abroad showing that CKDu is caused by glyphosate.”
NASSL President Prof Vijaya Kumar said: “The very limited information available on glyphosate in Sri Lanka does not show that levels of glyphosate in drinking water in CKDu affected areas (North Central Province) are above the international standards set for safety. CKDu is rarely reported among farmers in neighbouring areas such as Ampara, Puttlam and Jaffna or even the wet zone, where glyphosate is used to similar extent. It has also not been reported in tea growing areas where glyphosate is far more intensively used.”
Agrochemical regulation
In recent years, the search for CKDu causes has become too mixed up with the separate case for tighter regulation of agrochemicals, a policy need on its own merit. International experience shows that a sectoral approach works better than a chemical by chemical one.
The bottomline: improving Sri Lanka’s agrochemical regulation needs an evidence-based, rigorous process that does not jeopardize the country’s food security or farmers’ livelihoods. A gradual shift to organic farming (currently practiced on less than 2% of our farmland) is ideal, but can take decades to accomplish.
Our health and environmental activists must rise above their demonise-and-ban approaches to grasp the bigger picture. They can do better than ridiculing senior scientists who don’t support populist notions. Effective policy advocacy in today’s world requires problem solving and collaboration – not conspiracy theories or confrontation.
Hijacking a human tragedy like CKDu for scoring cheap debating points is not worthy of any true activist or politician.
CKDu was first reported in the early 1990s from a single Province in Sri Lanka’s heartland of rice farming, but it has now spread across approximately 17,000 sq km (a quarter of the island). An estimated 20,000 to 22,000 persons have died since the disease was identified. Several thousand more are living with the disease, on medication and (in advanced stages) receiving regular kidney dialysis.
Investigating causes of this ailment — still not pinned down to a specific cause or factor — has been difficult. While scientists follow rigorous scientific methods, ultra-nationalists and politicians trying to hijack the issue for their own agenda setting. Some journalists have added fuel to the fire with sensationalist reporting and fear-mongering.
In this update, I share findings of the National CKDu Research Project carried out by the Ministry of Health of the Lankan government with technical assistance from World Health Organisation, WHO. It was academically published in Aug 2013.
See also my other writing on the subject (some early ones are updated in this latest Ravaya column):
Villagers carry coffin containing body of Seneviratnalage Jayatillake, Lankan farmer who suffered from a mystery kidney disease, during his funeral in Padaviya Sri Lanka – Photo by Eranga Jayawwaardena, Associated Press
I am not a public health or environmental expert, but have long covered related topics as a science journalist.
Among my long-standing interests are the downstream health and environmental effects agrochemicals – both chemical fertilizers and farm chemicals applied against pests and weeds. Parallel to this, I have also been covering chronic kidney disease of uncertain aetiology (CKDu), a mysterious illness that has been affecting thousands of Lankan farmers for nearly 25 years.
A link between agrochemicals and CKDu is suspected, but not yet scientifically proven (even though environmentalists ask us to believe so). It is a current yet contentious topic, which I chose for my presentation to an international workshop on “Pesticides and Global Health: Research, Collaboration and Impact” held at the Department of Anthropology, University of Durham, UK, on 10 – 11 February 2015.
In my presentation, I explore the topic from the angle of public perceptions, which are largely shaped by what appears in the media. This has been problematic since mass kidney failure in Sri Lanka has been compounded by what I call a ‘mass media failure’.
Most of our media have failed to understand, analyse and report adequately on this public health emergency. Instead of helping affected people and policy makers to work out solutions, some journalists have become amplifiers of extreme activist positions. This has led to alarmism and policy confusion.
What is to be done? There are no short-cuts to the scientific investigation process which must follow – that means further research is needed to find definitive evidence for causative factors. That could take a while, given how people are exposed to multiple environmental, lifestyle and genetic factors.
But meanwhile, the welfare of those already affected by the disease and their families needs to receive greater public support. Environmentalists trying to score points from this tragedy overlook this vital humanitarian aspect.
A few excerpts from the presentation below. See full presentation above.
Advocacy journalism is fine; activist journalism is questionableWe need Lankan media to be more reflective, less accusatorySpare a thought for today’s policy-makers who must think and act on the run…
As a science journalist, I have been covering scientific aspects of the public health emergency of mass kidney failure that has killed an estimated 20,000 persons in Sri Lanka over the past two decades.
It emerged in the early 1990s, when hundreds of people in Sri Lanka’s Dry Zone – heartland of its farming — developed kidney failure without having the common causative factors of diabetes or high blood pressure.
Most affected were men aged between 30 and 60 years who worked as farmers. The disease built up inside the body without tell-tale signs or symptoms, manifesting only in advanced stages.
Over the years, many scientific studies have been carried out on what causes this mysterious disease, now called Chronic Kidney Disease of unknown aetiology, or CKDu. Various environmental, geochemical and lifestyle related factors have been probed. Researchers now suspect environmental and genetic factors as causes – but a definitive link to a specific factor has yet to be found.
On 23 January 2015, I answered a few questions posed by BBC World Service (radio) on CKDu, to feed a news report they were producing for global broadcast.
My full answers are shared here in the public interest.
Science writer Nalaka Gunawardene responds to questions from BBC World Service on the mysterious mass kidney failure in Sri Lanka: 23 January 2015
Question 1: What are the various theories that scientists have put forward as a possible cause for this disease which has been studied for 20 years?
Question 2: As a science journalist, you’ve been tracking the research on this public health concern for some years. What do you think is most likely cause?
Question 3: The World Health Organisation supported research has suggested a link with agrochemical use. Don’t you think that such a link is likely?
Question 4: The new government of Sri Lanka has just pledged to give high priority to the kidney disease. What are the challenges faced by the government in dealing with this crisis?
High inputs to make high yields – at a heavy price
“For sure, the double-edged legacy of the Green Revolution which promoted high external inputs in agriculture must be critiqued. Past mistakes can be rectified at least now.
“However, corrections have to begin upstream by questioning macro-level policies. For example, for half a century, Lankan farmers have had a huge — 90 per cent — state subsidy on chemical fertilisers. This does not encourage thrifty use, yet successive governments have hesitated to fix the massive drain of taxpayer funds.
“Thus, mass kidney failure is more than just a public health emergency or environmental crisis. It is symptomatic of cascading policy failures in land care, water management and farming over decades.”
This is an excerpt from the first of a monthly series of analysis blogs (columns) I will be writing for SciDev.Net in 2014.
Titled “Going upstream for lasting kidney disease remedies“, the first essay looks at the broader implications of a chronic kidney disease that is spreading in India and Sri Lanka for which medical and other researchers still cannot pinpoint a specific cause.
I have been writing and broadcasting about this public health issue for sometime, and have listened (or interviewed) most key players on the Lankan side of the investigation. In this opinion essay, I look at the policy dilemmas and healthcare challenges posed by Chronic Kidney Disease of uncertain aetiology, or CKDu.
I argue: “There are no quick fixes. In searching for solutions, health and environmental activists must rise above their single-issue advocacy positions. They can bring grassroots concerns to national debates. Collaboration – not confrontation or conspiracy theories – is the need of the hour.
“Hijacking a human tragedy for scoring some debating points is not worthy of any true follower of Rachel Carson.”