In this week’s Ravaya column (in Sinhala, appearing in issue dated 8 March 2015), I revisit a public health emergency that I also commented on in August/Sept 2012: Chronic Kidney Disease of unknown/uncertain etiology (abbreviated as CKDu).
CKDu was first reported in the early 1990s from a single Province in Sri Lanka’s heartland of rice farming, but it has now spread across approximately 17,000 sq km (a quarter of the island). An estimated 20,000 to 22,000 persons have died since the disease was identified. Several thousand more are living with the disease, on medication and (in advanced stages) receiving regular kidney dialysis.
Investigating causes of this ailment — still not pinned down to a specific cause or factor — has been difficult. While scientists follow rigorous scientific methods, ultra-nationalists and politicians trying to hijack the issue for their own agenda setting. Some journalists have added fuel to the fire with sensationalist reporting and fear-mongering.
In this update, I share findings of the National CKDu Research Project carried out by the Ministry of Health of the Lankan government with technical assistance from World Health Organisation, WHO. It was academically published in Aug 2013.
See also my other writing on the subject (some early ones are updated in this latest Ravaya column):
2 Sep 2012: සිවුමංසල කොලූගැටයා #81: වකුගඩු රෝගයේ විද්යාව හා විජ්ජාව
9 Sep 2012: සිවුමංසල කොලූගැටයා #82: රසායනික පොහොර ‘දෙවොලේ’ සිරගත වූ අපේ ගොවියා
3 Nov 2012:
18 August 2012: When Worlds Collide #29: Science and Politics of Kidney Disease in Sri Lanka
28 Dec 2013: Don’t exaggerate Lanka’s kidney disease, its discoverer pleads
23 January 2014: SciDev.Net: Going upstream for lasting kidney disease remedies
25 January 2015: Mysterious Kidney Disease in Sri Lanka: Nalaka Gunawardene answers BBC’s questions
15 Feb 2015: Public perceptions of pesticides & how they influence policy: Case of CKDu in Sri Lanka
නිදන්ගත වකුගඩු රෝගය මෙරට ප්රධානතම මහජන සෞඛ්ය ගැටලූවක් හා ප්රතිපත්තිමය අභියෝගයක් බවට පත් වී තිබෙනවා. මෙයට වඩාත් විධිමත් ප්රතිචාර දැක්වීමේ හදිසි අවශ්යතාව නව ජනාධිපතිවරයාත්, සෞඛ්ය අමාත්යවරයාත් මෑතදී අවධාරණය කළා.
මේ ගැන කථා කරන හැම විටම අප සිහි තබා ගත යුතු වැදගත් මූලික කරුණක් තිබෙනවා. අද සෞඛ්ය ක්ෂේත්රයට ප්රබල ප්රශ්නයක් වී ඇත්තේ නිශ්චිත හේතුකාරකයක් හඳුනා නොගත් වකුගඩු රෝගය බවයි (Chronic Kidney Disease of uncertain aetiology, CKDu).
සාමාන්යයෙන් වකුගඩු ආසාදනය වීමට අධික රුධිර පීඩනය, දියවැඩියාව, ජානමය සාධක, (බටහිර ක්රමයේ හෝ දේශීය ක්රමයේ) සමහර බෙහෙත් අනිසි භාවිතය ආදී හේතුකාරක මුල් වනවා. මේ දන්නා හේතු නිසා වකුගඩු රෝගී වූ අය සැළකිය යුතු පිරිසක් මෙරට සිටිනවා. ඇත්තටම සංඛ්යාත්මකව බහුතරය ඔවුන්.
ඒ අතර 1990 දශකය මුල සිට වියළි කලාපයේ ප්රදේශවලින් වාර්තා වූ අසාමාන්ය ආකාරයේ වකුගඩු රෝගයට මේ දන්නා සාධක බලපා නැහැ. එයට තුඩු දෙන්නේ කුමක්දැයි සොයා විද්යාත්මක පර්යේෂණ රැසක් සිදු කොට තිබෙනවා.
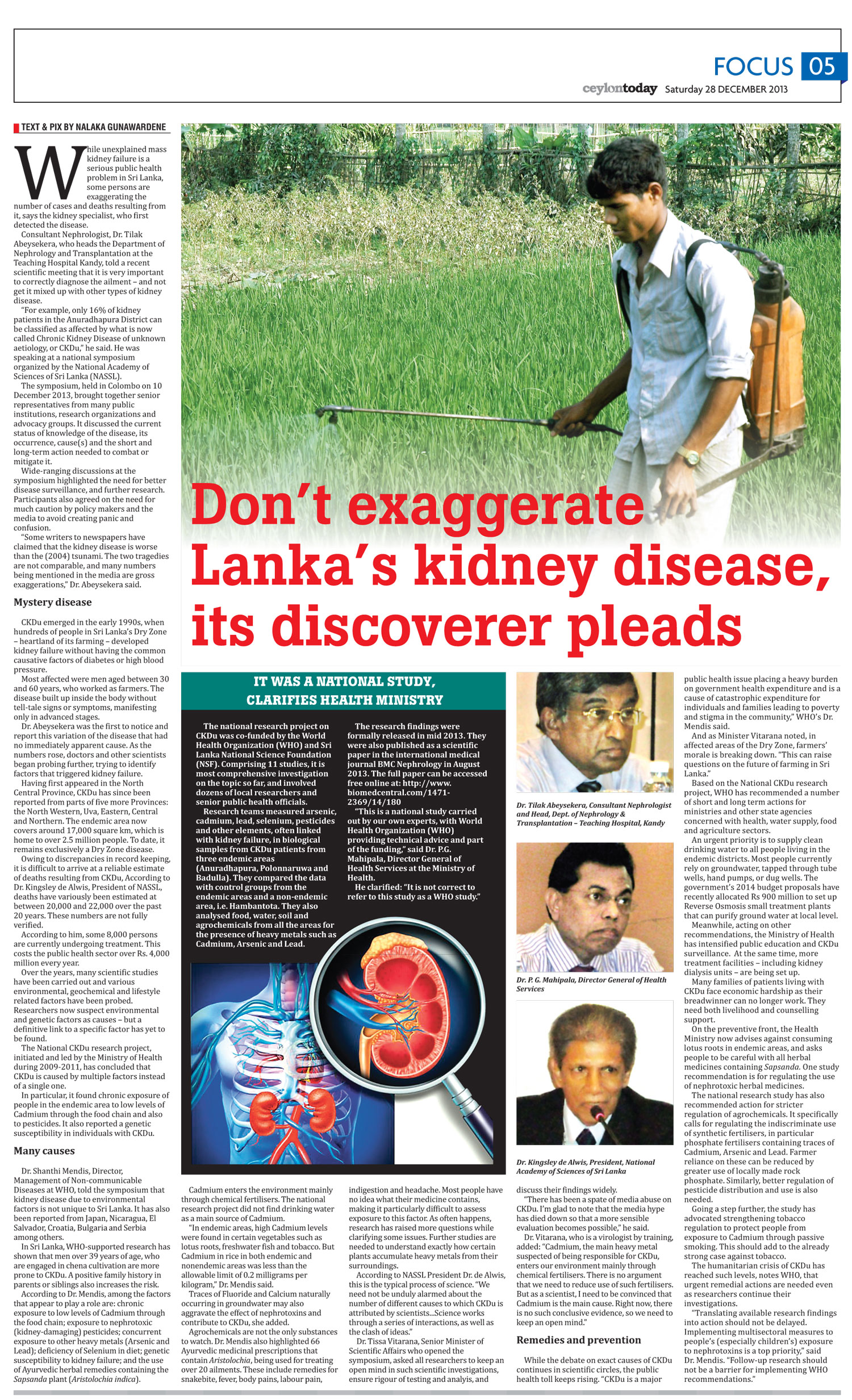
මේ හේතු නොදන්නා වකුගඩු රෝගය මුල් වරට හඳුනා ගත් වකුගඩු විශේෂඥයා, වෛද්ය තිලක් අබේසේකර. මීට මාස කිහිපයකට පෙර කොළඹ පැවති ජාතික විද්යා ඇකඩමිය සංවිධානය කළ මේ පිළිබඳ ජාතික සමුළුවකදී ඔහු ප්රබල ඉල්ලීමක් කළා.

‘‘දෙආකාරයක වකුගඩු ආසාදන අප රටේ දැන් හමු වනවා. මේ දෙවර්ගය පටලවා නොගෙන වෙන් වශයෙන් හඳුනා ගැනීම ඉතා වැදගත්. උදාහරණයකට මා දන්නා පරිදි අනුරාධපුර දිස්ත්රික්කයේ වකුගඩු රෝගීන් අතරින් හේතුව නොපැහැදිලි වකුගඩු රෝගයෙන් පෙළෙන්නේ 16%ක් පමණ සංඛ්යාවක්.’’
වෛද්ය අබේසේකර කනගාටුවෙන් කියා සිටියේ පුවත්පත්වලට ලිපි ලියන ඇතැම් දෙනා මේ වෙනස නොදැන හෝ නොසලකා හැර තත්ත්වය සැබෑවට වඩා වැඩිකොට දක්වන බවයි.
‘‘සමහරු මෙය 2004 සුනාමියටත් වඩා බිහිසුණු යැයි කියනවා. මාධ්යවල මේ රෝගය ගැන සඳහන් කැරෙන බොහෝ සංඛ්යා ලේඛන අතිශයෝක්තීන්. මෙසේ කිරීමෙන් මේ රෝගය හරිහැටි තේරුම් ගැනීමට හා ප්රතිචාර දැක්වීමට තිබෙන වෛද්ය හා සෞඛ්ය බලධාරීන්ට තිබෙන අවකාශය ඇසිරෙනවා. අනවශ්ය බියක් හා කලබලයක් ඇති කෙරෙනවා.’’
CKDu රෝගය හඳුනාගත් කාලයේ සිට මේ වන තුරු මිය ගිය සංඛ්යාව පිළිබඳව නිවැරදි ගණනයක් ද නැහැ. වසර 25කට ආසන්න කාලයක් තුළ එය 20,000 – 22,000 අතර බවට අනුමාන කෙරෙනවා. රෝගයත් සමඟ ජීවත් වන හා ප්රතිකාර ලබන සංඛ්යාව 2013 අගදී 8,000ක් පමණ බව වෛද්ය අබේසේකර ප්රකාශ කළා.
2010දී සෞඛ්ය අමාත්යාංශය මේ රෝගය ගැන ජාතික පර්යේෂණයක් දියත් කළා (National CKDu research project). මෙහි මුලික අරමුණ වූයේ රෝගයේ ගති සොබා අධ්යයනය කිරීම, හේතුකාරක හඳුනාගැනීම, හා වළක්වා ගැනීමේ ක්රමවේදයන් නිර්ණය කිරීමයි.
විවිධ විද්යා ක්ෂේත්රයන්ගේ විද්වත් දායකත්වය ලබා ගත් මේ පර්යේෂණයට ලෝක සෞඛ්ය සංවිධානයේ (WHO) සහයෝගය ලබා ගත්ත ද එය WHO පර්යේෂණයක් නොව ශ්රී ලංකා ජාතික ව්යායාමයක් බව සෞඛ්ය අමාත්යාංශය අවධාරණය කරනවා.
එහිදී අනුරාධපුර, පොළොන්නරුව හා බදුල්ල දිස්ත්රික්ක තුනට විශේෂ අවධානය යොමු කෙරුණා. රෝගීන්ගෙන් ලබා ගත් මුත්රා හා රුධිර සාම්පල, නියපොතු හා කෙස්වල වකුගඩුවලට හානි කළ හැකි බැරලෝහ (ආසනික්, කැඞ්මියම්, ඊයම්) ඇත්දැයි පරීක්ෂා කරනු ලැබුවා. කෘෂිරසායන ශේෂයන් (agrochemical residues) සඳහා ද රසායනාගාර පරීක්ෂා කරනු ලැබුවා. රෝගය වාර්තා වී නැති හම්බන්තොට දිස්ත්රික්කයේ පුද්ගලයන්ගෙන් ලබා ගත් සාම්පල සමග සන්සන්දනය කෙරුණා.
එසේම මේ දිස්ත්රික්ක හතරේම ළිංවලින්, නල ළිංවලින්, සොබාවික උල්පත්වලින් හා වාරි ඇළ මාර්ගවලින් ජල සාම්පල එකතු කොට පරීක්ෂා කෙරුණා. මේ ප්රදේශවල පස් සාම්පල, ආහාර බෝග හා වල්පැළෑටි සාම්පල එකතු කොට ඒවායේ බැරලෝහ අන්තර්ගතය ද පිරීක්සනු ලැබුවා. මීට අමතරව ෆොස්ෆේට් පොහොර, වල්නාශක හා කෘමිනාශකවල බැර ලෝහ ප්රමාණයන් සාම්පල් හරහා පරීක්ෂා කෙරුණා.
මේ පුළුල් වූත්, ක්රමානුකූල වූත් පරීක්ෂාවන් සිය ගණනකින් මතු වූ දත්ත සංඛ්යාලේඛන විද්යාවේ මූලධර්මවලට අනුකූලව සියුම් ලෙස විශ්ලේෂණය කෙරුණා.
මේ සියල්ල විස්තරාත්මකව 2013 අගෝස්තු මාසයේ BMC Nephrology නම් ජාත්යාන්තර වෛද්ය විද්යා පර්යේෂණ සඟරාවේ විද්යාත්මක නිබන්ධයක් ලෙස ප්රකාශයට පත් කරනු ලැබුවා. මෙය මෙම වෙබ් අඩවියෙන් කියවිය හැකියි.
http://www.biomedcentral.com/1471-2369/14/180

දේශීය විද්යාඥයන් දුසිම් ගණනකගේ සහභාගීත්වය පැවති CKDu ජාතික පර්යේෂණ කණ්ඩායම වෙනුවෙන් මේ පර්යේෂණ නිබන්ධයට කර්තෘ බව දී තිබුණේ සෞඛ්ය අමාත්යාංශයේ ජ්යෙෂ්ඨ නිලධාරීන් වූ වෛද්ය නිහාල් ජයතිලක හා වෛද්ය පාලිත මහීපාලත්, ලෝක සෞඛ්ය සංවිධානයේ දේශීය නියෝජිත වෛද්ය ෆිර්ඩෝසි ආර්. මේතා සහ ජීනීවා මූලස්ථානයේ බෝනොවන රෝග පිළිබඳ අංශයේ වෛද්ය ශාන්ති මෙන්ඩිස් යන සිවු දෙනායි.
නිබන්ධය අවසානයේ ඔවුන් නිගමනය ලෙස මෙසේ කියනවාථ ‘‘CKDu නිදන්ගත වකුගඩු රෝගයට දායක වන හේතුකාරකයන් ගණනාවක් පැවතිය හැකි බව පෙනී යනවා. අප සොයා ගත් කරුණුවලට අනුව පැළෑටි මත පදනම් වූ ඖෂධ ගැනීම හෝ (බටහිර) වේදනානාශක ඖෂධ අනිසි ලෙස ගැනීම හෝ මෙම රෝගයට හේතුවන්නේ යැයි සිතිය නොහැකියි.’’
‘‘අපේ ප්රතිඵලවලට අනුව මේ රෝගය හමුවන ප්රදේශවල ජනයා දිගු කාලීනව සිය ආහාර හරහාත්, කෘමිනාශක හරහාත් කැඞ්මියම් බැර ලෝහයේ අඩු මට්ටම්වලට නිරාවරණය වී තිබෙනවා. මීට අමතරව මේ ජනයා ඊයම් හා ආසනික් ලෝහවලට ද ආහාර හරහා නිරාවරණය වී තිබිය හැකියි. රෝගීන්ගේ මුත්රා සාම්පල්වල තිබූ කැඞ්මියම් හා ආසනික් මට්ටම් වකුගඩුවලට හානි කරන මට්ටමේ වූවා. විශේෂයෙන්ම කැඞ්මියම් බැර ලෝහය මෙරට නිදන්ගත වකුගඩු රෝගයට හේතුවක් විය හැකි අවදානම් සාධකයක් (risk factors) බව පෙනෙනවා. මීට අමතරව සෙලීනියම් පෝෂණ ඌණතාවය හා පාරම්පරිකව ජානමය වශයෙන් වකුගඩු රෝගීන් වීමේ වැඩි නැඹුරුවක් පැවතීමද මෙකී රෝගය හට ගැනීමට තුඩු දිය හැකි යැයි විශ්වාස කළ හැකියි.’’
නිබන්ධය පුරාම ඔවුන් කියන්නේ තව දුරටත් විවිධ කෝණයන්ගෙන් මේ රෝගය විද්යාත්මකව අධ්යයනය කිරීමේ වැදගත්කමයි. මිනිස් දේහය එකවර ආහාර, පාන, ආශ්වාස වාතය හා වෙනත් ක්රම හරහා බහුවිධ බලපෑම්වලට පත්වන බැවින් එක් රෝගයකට හේතු වන සාධකයක් නිශ්චිතව වෙන් කර තහවුරු කර ගැනීමේ අපහසුතාවට මේ පර්යේෂකයන් මුහුණ දුන්නා.
මේ සීමාවන් තුළ අවදානමක් මතු කරන හෝ තීව්ර කරන සාධක මොනවාදැයි හඳුනා ගැනීමේ උත්සාහයක් තිබුණා. විශේෂයෙන් රෝගයෙන් පෙළෙන අයගේ සාම්පල්වල කැඞ්මියම් මට්ටම් වඩා ඉහළ වීම සැලකිය යුතුයි. එසේම කැඞ්මියම් හා ආසනික් ලෝහ දෙකට එකවර නිරාවරණය වූ විට ඒ එකක් තනි තනිව ශරීරගත වීමට වඩා දිගු කාලීන බලපෑමක් කරන බවද පෙනෙනවා.
සෙලිනියම් යනු අපේ ශරීරයට මඳ වශයෙන් අවශ්ය අංශුමාත්ර මූලද්රව්යයක් (ක්ෂුද්ර පෝෂකයක්). ශරීරයට සෙලිනියම් ලැබෙන්නේ බිත්තර, මාළු, මස්, හතු වර්ග හා සමහර ඇට වර්ග හරහායි. ස්වාභාවික වකුගඩු සිරුර තුළ රැක ගැනීමේදී ශරීරගත සෙලීනියම් මට්ටම උපකාර වන බවත්, මෙම පරීක්ෂාවලට ලක් වූ රෝගීන්ගේ සෙලීනියම් ඌණතා පැවතීම හරහා එම ආරක්ෂාව ඔවුන් නොලද බවත් පර්යේෂකයෝ කියනවා.
පොදුවේ හඳුනා ගත් ප්රවණතාවක් නම් නිදන්ගත වකුගඩු රෝගය හට ගන්නේ භූගත ජලය පානයට ගැනීම බහුලව සිදුවන ප්රදේශවල ජනයාට බවයි. මේ ප්රදේශවල භූගත ජලයේ ස්වභාවය කැල්සියම් හා ෆ්ලෝරයිඞ් මට්ටම් ඉහළයි. ඓතිහාසිකව ජනයා මේ ජලය පානය කළද වකුගඩු රෝගයක් වාර්තා වී තිබුණේ නැහැ. එහෙත් වඩා මෑත කාලයේ ආහාරපාන රටා වෙනස්වීම, ජලයේ ඛනිජ ප්රමාණය වැඩිවීම, අධික උණුසුම් පරිසරයක ඇති තරම් ජලය දිනපතා පානය නොකිරීම ආදී සාධක ගණනාවක සංකලනය මේ ප්රදේශවාසීන්ට නිදන්ගත වකුගඩු රෝගය සෑදීමේ ඉඩ වැඩි කළාද?
මෙම ප්රදේශවල පරීක්ෂා කළ එළවළුවල හා මසුන්ගේ කැඞ්මියම් හා ඊයම් මට්ටම් ජාත්යන්තරව නිර්දේශිත උපරිම මට්ටම්වලට වඩා ඉහළින් පැවතියා. ඒ කියන්නේ මිනිස් සිරුරට නුසුදුසු තරම් බැර ලෝහ ආහාර හරහා නිරායාසයෙන්ම ශරීරගත වන බවයි. මේ කැඩ්මියම් එන්නේ කොහි සිටද?
නිදන්ගත වකුගඩු රෝගයන් ලෝකයේ වෙනත් රටවලින් ද වාර්තා වී තිබෙනවා. එම රටවල එයට දක්වන ප්රතිචාරවලින් ශ්රී ලංකාවට ද ආදර්ශ ගත හැකි බව CKDu ජාතික පර්යේෂණය කළ විද්වතුන් කියනවා. විශේෂ අවධානයක් යොමු කළ යුතු පියවර නම්:
- එම ප්රදේශවල සියලූ ජනයාට පිරිසිදු පානීය ජලය ලැබීමට සැලැස්වීම.
- රසායනික පොහොර ඇතුලූ සියලූ කෘෂිරසායනික නිසි නියාමනයක් හා අධීක්ෂණයක් යටතේ භාවිතය.
- බැර ලෝහ අඩංගු බැටරි භාවිතයෙන් පසු ඉවත දැමීමේදී පරිසරය දුෂණය විය හැකි ලෙස මුදා නොහැරීම.
- දුම්පානය හා වකුගඩු රෝග අතර ඍජු සබඳතාවක් සොයා ගෙන ඇති බැවින්, දුම්කොළ පාලනය.
- බැර ලෝහ සමහරක් වාත දුෂණය හරහා ආශ්වාස කිරීම සිදු වන නිසා වාත දුෂණය පාලනය කිරීම.
මෙයින් පෙනී යන්නේ සරල තනි පියවරක් නොව පොදුවේ මහජන සෞඛ්යයට හිතකර වන පියවර රැසක් ගත හැකි හා ගත යුතු බවයි.
CKDu ජාතික පර්යේෂණයේ ප්රතිඵල වාර්තාව පදනම් කර ගෙන සෞඛ්ය අමාත්යාංශය අදාළ පාර්ශවයන්ගේ සහයෝගයෙන් විවිධ පියවර ගැනීම අරඹා තිබෙනවා.
‘‘කෘෂිකර්ම අමාත්යාංශය, වාරිමාර්ග දෙපාර්තමේන්තුව, විද්යා හා තාක්ෂණ ආයතන, සමාජසේවා රාජ්ය ආයතන ආදියේ සහභාගීත්වය ඇතිව අප උත්සාහ කරන්නේ අපේ රටේ ජනතාව වකුගඩුවලට හානි කරන සාධකවලට නිරාවරණය වීම හැකිතාක් අවම කිරීමටයි. නිදන්ගත වකුගඩු රෝගය හමු වන ප්රදේශවල ජල සැපයුම විධිමත් කිරීමටත්, රසායනික පොහොර හා කෘමිනාශක රටට ලබා ගැනීම හා රට තුළ බෙදා හැරීම වඩා හොදින් නියාමනය කිරීමටත් පියවර ගනු ලබනවා’’ යැයි පර්යේෂණ නිබන්ධය අවසානයේදී එහි කතුවරුන් ප්රතිඥාවක් දෙනවා.

Sri Lanka – Photo by Eranga Jayawwaardena, Associated Press
මෙම රෝගයට ප්රතිචාර දැක්වීමේදී සෞඛ්ය අමාත්යංශය පෙරටු කරගත් සමස්ත ලාංකික රාජ්ය තන්ත්රය හා ලක් සමාජයටම විශාල අභියෝගයක් වන්නේ රෝගකාරක සාධකය නිශ්චිත ලෙස හඳුනාගන්නා තුරු බලා නොසිට ප්රතිකාර මෙන්ම වැළැක්වීමේ ක්රමෝපායන් ක්රියාත්මක කිරීමයි.
2013 වන විට මෙරට සෞඛ්ය සේවා සඳහා රජය වාර්ෂිකව වෙන් කෙරෙන මහජන මුදල්වලින් 5%ක් පමණ මෙම රෝගයෙන් පෙළෙන අයට ප්රතිකාර කිරීමට වැය කෙරුණා. රෝගයේ උත්සන්න අවස්ථාවලට එළැඹි විට සතියකට 3-4 වතාවක් රුධිරය කාන්දු පෙරීම (kidney dialysis) අවශ්යයි. මේ සඳහා යොදා ගන්නා යන්ත්ර මුළු රටේම රාජ්ය රෝහල් පද්ධතියේ ඇත්තේ 200කට අඩු සංඛ්යාවක්.
රෝගීන්ට ප්රතිකාර කිරීමට අවශ්ය යටිතල පහසුකම් ප්රමාණවත් නොවීම නිසා සෞඛ්ය සේවා පීඩනයට ලක්ව තිබෙනවා. බොහෝ රෝගීන්ට හා ඔවුන්ගේ පවුල්වලට පෞද්ගලික රෝහලකින් රුධිර කාන්දු පෙරීම සිදුකරගන්නට වත්කමක් නැහැ. (එබඳු එක් සැසිවාරයකට රු. 12,000ක් පමණ වැය වනවා.)
රෝගයට ලක් වූ පවුල් සාමාජිකයා බොහෝ විට පවුලේ ප්රධාන හෝ එකම ආදායම් උපදවන්නායි. මේ නිසා රෝගීන්ගේ පවුල් ආර්ථික වශයෙනුත්, ඉනික්බිති මානසිකව හා සාමාජයීය ලෙසත් මහත් පීඩාවට පත්වනවා.
මෙය සෙමෙන් දිග හැරෙන මානුෂික ඛේදවාචකයක්. මේ ව්යසනයට මුහුණ දී සිටින පවුල් දහස් ගණනක් සිටිනවා. මෙයට ප්රතිචාර දැක්වීම හා රෝගීන් රැක බලා ගැනීම හුදෙක් රජයට පමණක් කළ හැකි දෙයක් නොවෙයි. පෞද්ගලික අංශය, ස්වේච්ඡා ආයතන, විද්වත් කණ්ඩායම් ඇතුලූ සමාජයේ සැමට මෙම සුබසාධනයේ කොටස්කරුවන් විය හැකියි.
මේ මානුෂික ප්රශ්නය තමන්ගේ පටු න්යායපත්රවලට අමතර තර්කයක් බවට හරවා ගත් සමහර අන්තවාදී පරිසරවේදීන් හා දේශපාලන ක්රියාකාරිකයන් ද සිටිනවා. ඔවුන්ගේ ප්රකාශ හා උද්ඝෝෂණ නිසා මේ අභියෝගය හරිහැටි තේරුම් ගෙන එයට ප්රතිචාර දැක්වීම ව්යාකූල වී තිබෙනවා. ඒ ගැන මීළඟ සතියක කථා කරමු.